

Association between nasopharyngeal airway lipidome signatures of infants with severe bronchiolitis and risk of recurrent wheeze: A prospective multicenter cohort study
- PMID: 39503262
- PMCID: PMC11807286
- DOI: 10.1111/pai.14274
Association between nasopharyngeal airway lipidome signatures of infants with severe bronchiolitis and risk of recurrent wheeze: A prospective multicenter cohort study
Abstract
Background: Infants hospitalized for bronchiolitis are at high risk for developing recurrent wheeze in childhood. The role of airway lipids in the link between these two conditions remains unclear. This study aimed to identify the association between airway lipids in infants hospitalized for bronchiolitis and the development of recurrent wheeze, with a focus on immunoglobulin E (IgE) sensitization.
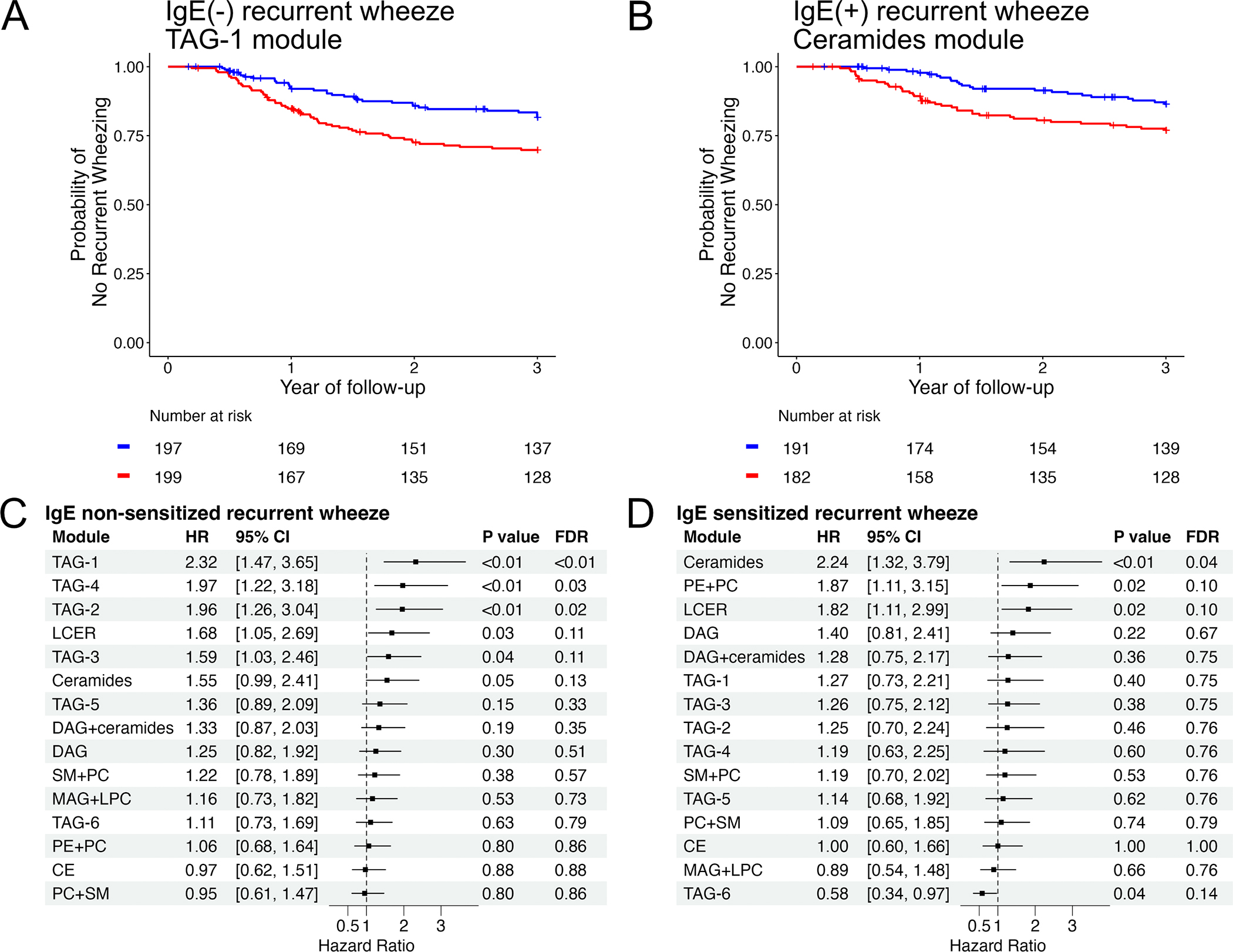
Methods: In a multicenter prospective cohort study of 919 infants (age <1 year) hospitalized for bronchiolitis, we performed lipidomic profiling of nasopharyngeal airway specimens collected at hospitalization. We first identified lipid modules composed of highly correlated lipids by performing weighted correlation network analysis. We then examined the longitudinal association of those lipid modules with the rate of recurrent wheeze by age 3 years after discharge from hospitalization for bronchiolitis. We also examined the associations of lipid modules with IgE non-sensitized (i.e., neither sensitized at admission nor at age 3 years) and IgE-sensitized (i.e., sensitized at admission and/or at age 3 years) recurrent wheeze by age 3 years, respectively.
Results: Our analysis identified 15 distinct lipid modules in the nasopharyngeal airway lipidome data. Overall, lipid modules composed of triacylglycerols (hazard ratio [HR] 1.78, 95% confidence interval [CI] 1.26-2.51, FDR < 0.01) and sphingolipids (HR 1.74, 95% CI 1.25-2.44, FDR <0.01) had the strongest associations with recurrent wheeze development. Stratification by IgE sensitization revealed differential associations. For example, the module composed of triacylglycerols was significantly associated with IgE non-sensitized recurrent wheeze, whereas the module composed of sphingolipids was significantly associated with IgE-sensitized recurrent wheeze (both FDR <0.05).
Conclusion: Distinct nasopharyngeal airway lipid modules are associated with recurrent wheeze development following severe bronchiolitis, with different patterns based on IgE sensitization status.
Keywords: airway; bronchiolitis; immunoglobulin E; infants; lipidomics; wheezing.
© 2024 European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
Figures




References
-
- Wolters AAB, Kersten ETG, Koppelman GH. Genetics of preschool wheeze and its progression to childhood asthma. Pediatr Allergy Immunol. 2024;35(1):e14067. - PubMed
-
- Marlow R, Finn A, Henderson J. Assessing the association between bronchiolitis in infancy and recurrent wheeze: a whole English birth cohort case-control study. Thorax. 2019;74(5):503–505. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AI127507/AI/NIAID NIH HHS/United States
- R01 AI148338/AI/NIAID NIH HHS/United States
- U01 AI087881/AI/NIAID NIH HHS/United States
- R01 AI137091/AI/NIAID NIH HHS/United States
- K01 AI153558/AI/NIAID NIH HHS/United States
- UG3 OD023253/OD/NIH HHS/United States
- American Lung Association
- Harvard University
- Massachusetts General Hospital
- R01 AI134940/AI/NIAID NIH HHS/United States
- R01 AI114552/AI/NIAID NIH HHS/United States
- UH3 OD023253/OD/NIH HHS/United States
- Japanese Dermatological Association
- Japan Society for the Promotion of Science
- International Medical Research Foundation
LinkOut - more resources
Full Text Sources
