

Frequency and clinical characteristics of children and young people with type 2 diabetes at diagnosis from five world regions between 2012 and 2021: data from the SWEET Registry
- PMID: 39503771
- PMCID: PMC11663186
- DOI: 10.1007/s00125-024-06283-5
Frequency and clinical characteristics of children and young people with type 2 diabetes at diagnosis from five world regions between 2012 and 2021: data from the SWEET Registry
Abstract
Aims/hypothesis: The diagnosis of type 2 diabetes is increasing in young people worldwide. This study evaluated the frequency and clinical characteristics of young people presenting with type 2 diabetes from the multinational SWEET e.V Registry 2012-2021, including the first years of the COVID-19 pandemic.
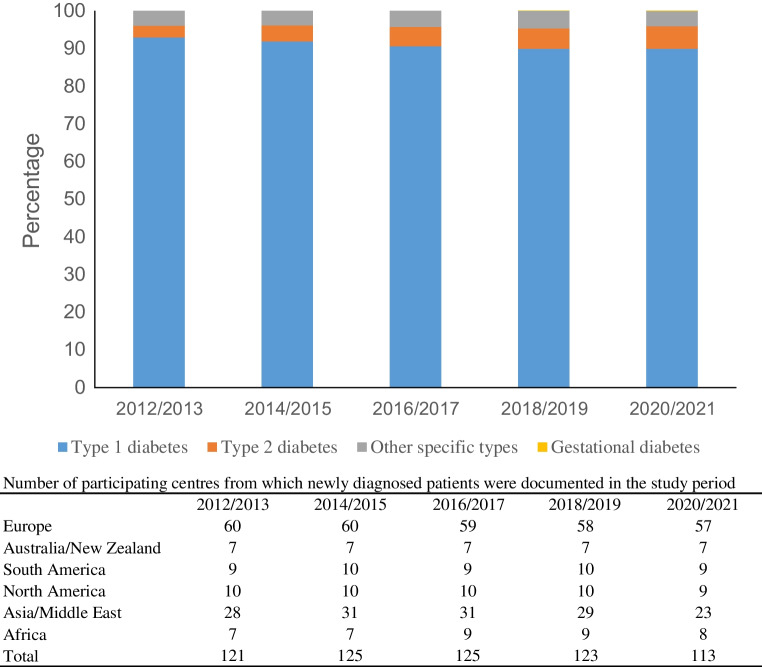
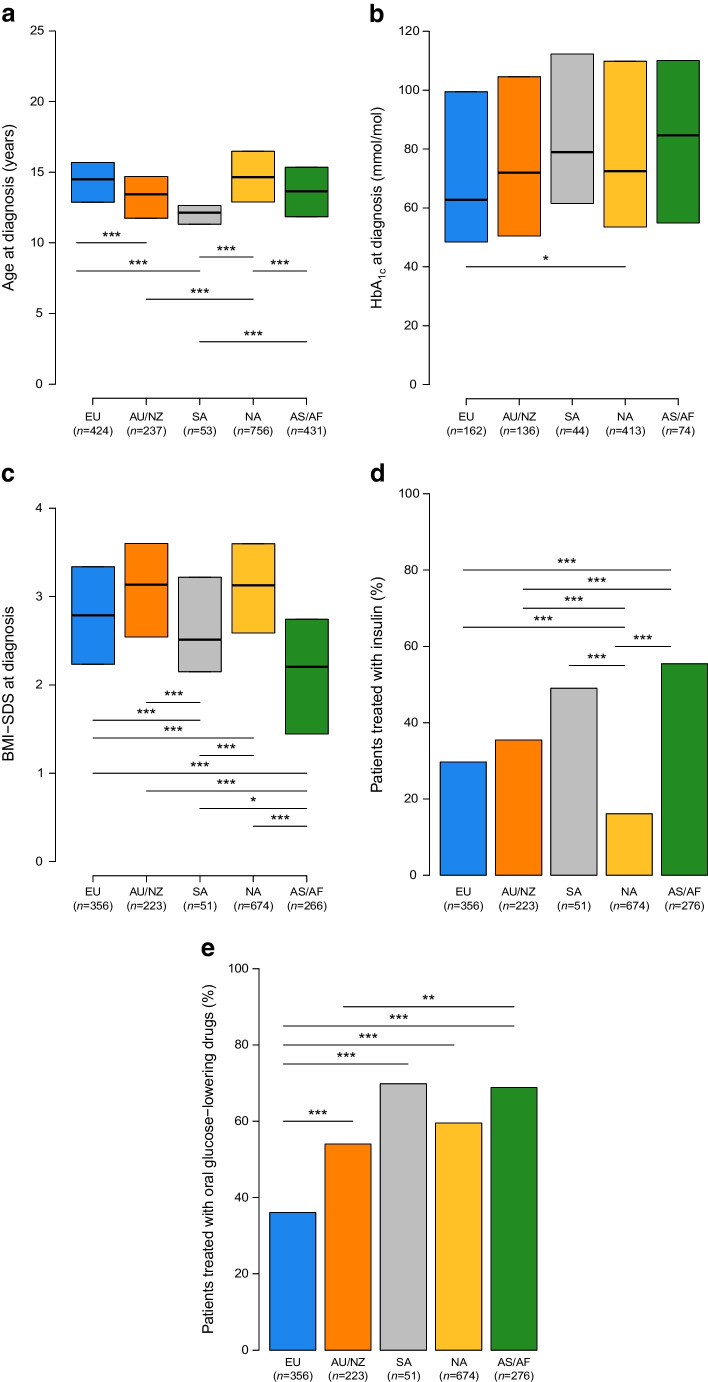
Methods: This is a longitudinal observational study based on the SWEET Registry, which collects demographic and clinical data on children and adolescents with diabetes from centres worldwide, with the diagnosis and classification of diabetes provided locally by each centre according to International Society for Paediatric and Adolescent Diabetes definitions. By July 2022, the SWEET Registry included 96,931 individuals from 130 centres with a total of 1,154,555 visits. Data were analysed by region: Europe (EU), Australia and New Zealand (AU/NZ), South America (SA), North America (NA) and Asia/Middle East and Africa (AS/AF). Trends in proportions for the two-year periods, calculated as cases with type 2 diabetes diagnoses over all cases with diabetes diagnoses, were estimated using logistic regression models adjusted for age at onset and sex.
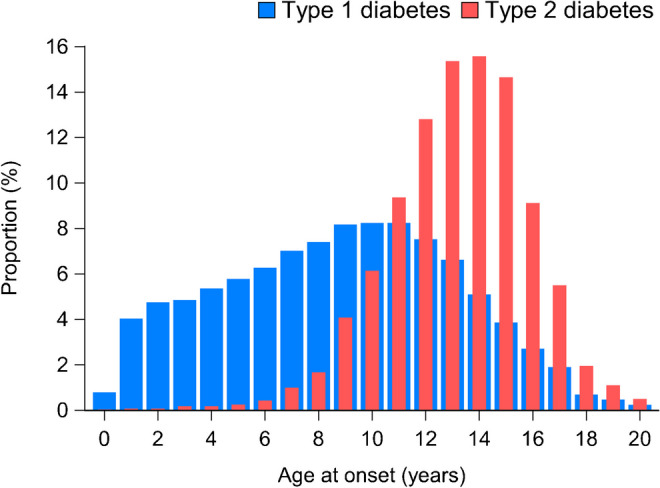
Results: Overall, there were 2819 of 58,170 new cases (4.8%) with type 2 diabetes: 614 in EU, 293 in AU/NZ, 79 in SA, 1211 in NA and 622 in AS/AF. The proportion of type 2 diabetes increased from 3.2% to 6.0% from 2012/2013 to 2020/2021, a relative rate of increase of 9% per two-year period (95% CI 5.9, 12.3; p<0.001). In the two-year period of the COVID-19 pandemic, type 2 diabetes continued to follow the observed trend, with a proportion of 6.0% in 2020-2021 compared with 5.4% in 2018-2019. High variability in the proportion of type 2 diabetes was observed across regions, with the lowest values observed in EU and the highest in NA. A significant increase in the proportion of type 2 diabetes was observed in EU, AU/NZ and NA. The median HbA1c was not uniform and was highest in AS/AF (85 mmol/mol [9.9%]; IQR 55-111 [7.2-12.3%]) and lowest in EU (63 mmol/mol [7.9%]; IQR 48-99 [6.5-11.2%]), and the difference between EU and NA (median value 73 mmol/mol [8.8%]; IQR 50-105 [6.7-11.8%]) was statistically significant (p=0.047). There was also a difference in BMI SD score by region: the lowest median BMI SD score was 2.2 (IQR 1.4-2.7) in AS/AF and the highest was 3.1 (IQR 2.5-3.6) in AU/NZ.
Conclusions/interpretation: The multinational SWEET data from the years 2012 to 2021 inclusive support recent findings of a worldwide increase in type 2 diabetes in young people, albeit with regional differences. This increase highlights the need for ongoing preventive measures and available advanced treatment modalities worldwide.
Keywords: Adolescents; Children; Geographical variability; Temporal trends; Type 2 diabetes.
© 2024. The Author(s).
Conflict of interest statement
Acknowledgements: The SWEET e.V. Registry is funded by the SWEET members, including the SWEET corporate members, namely Abbott, Boehringer Ingelheim, Dexcom, Insulet, Eli Lilly, Medtronic Europe, Novo Nordisk and Sanofi. The content of this work is solely the responsibility of the authors and does not necessarily represent the official views of the corporate members. The authors thank the following individuals for their support of this work: S. Tittel and S. Lanzinger for data management, and A. Hungele and R. Ranz for the SWEET-DPV software (all from Ulm University, Germany); M. Witsch (Centre Hospitalier de Luxembourg, Luxembourg), T. Danne and O. Kordonouri (Kinder- und Jugendkrankenhaus Auf Der Bult, Hannover, Germany) for centre integration; K. Klee and N. Koller (Kinder- und Jugendkrankenhaus Auf Der Bult) for initiating the SWEET collaboration; and S. Lanzinger and R. Holl (both Ulm University) for invaluable support. Finally, the authors thank all centres of the SWEET network, especially the collaboration centres that participated in this investigation. Parts of this study were presented in the oral presentation session at the 83rd Scientific Session of the American Diabetes Association (San Diego, 23–26 June 2023), and in the poster presentation session at the 57th European Diabetes Epidemiology Group annual meeting (Soesterberg, the Netherlands, 22–25 April 2023). Data availability: Access to the programming code may be provided by the corresponding author if requested. For reasons of data protection, data at the individual level cannot be provided. Funding: Open Access funding enabled and organized by Projekt DEAL. The SWEET Registry is a non-profit charity registered in Hannover, Germany. It is financed through membership fees from the participating centres (based on the income of the country of residence, according to the World Bank) and corporate members. We acknowledge with gratitude the support from the following SWEET corporate members (in alphabetical order): Abbott, Boehringer Ingelheim, Dexcom, Insulet, Eli Lilly, Medtronic Europe, Novo Nordisk and Sanofi. The SWEET project is an ongoing registered research collaboration (ClinicalTrials.gov registration number NCT04427189). Authors’ relationships and activities: The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work. Contribution statement: RG and VC designed the study, participated in data interpretation and wrote the manuscript. AJE performed the statistical analysis, participated in data interpretation, and reviewed and edited the manuscript. SB, NAC, FC, JK, CJ, EFG, AV, SS and SA researched data and reviewed and edited the manuscript. All authors approved the final version of the manuscript. RG, VC and AJE are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Figures


References
-
- FazeliFarsani S, van der Aa MP, van der Vorst MM, Knibbe CA, de Boer A (2013) Global trends in the incidence and prevalence of type 2 diabetes in children and adolescents: a systematic review and evaluation of methodological approaches. Diabetologia 56(7):1471–1488. 10.1007/s00125-013-2915-z - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
