

A phase 1/2 study of gilteritinib in combination with chemotherapy in newly diagnosed patients with AML in Asia
- PMID: 39503987
- PMCID: PMC11748473
- DOI: 10.1007/s12185-024-03840-x
A phase 1/2 study of gilteritinib in combination with chemotherapy in newly diagnosed patients with AML in Asia
Abstract
Objective: This interim analysis of a phase 1/2, open-label, single-arm study assessed the safety, efficacy, and pharmacokinetics of gilteritinib plus chemotherapy in adults with newly diagnosed FLT3 mutation-positive acute myeloid leukemia.
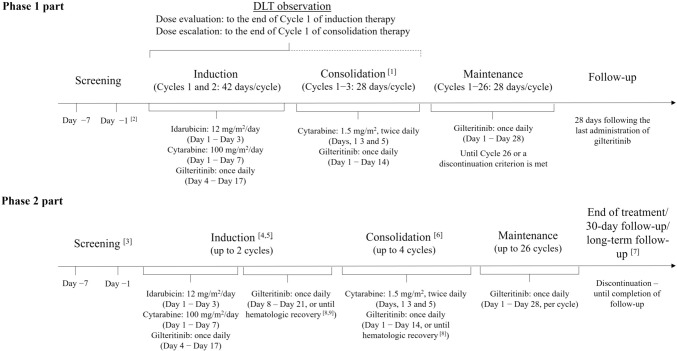
Methods: In sequential phase 1 and 2 studies, induction and consolidation therapy with gilteritinib 120 mg/day plus chemotherapy (induction: idarubicin/cytarabine once daily; consolidation: cytarabine twice daily) was followed by maintenance gilteritinib 120 mg/day monotherapy. Endpoints included maximum tolerated dose (MTD), recommended expansion dose (RED), and dose-limiting toxicity (phase 1), and complete remission (CR) rate following induction therapy (primary endpoint), overall survival (OS), safety, and pharmacokinetics (phase 2).
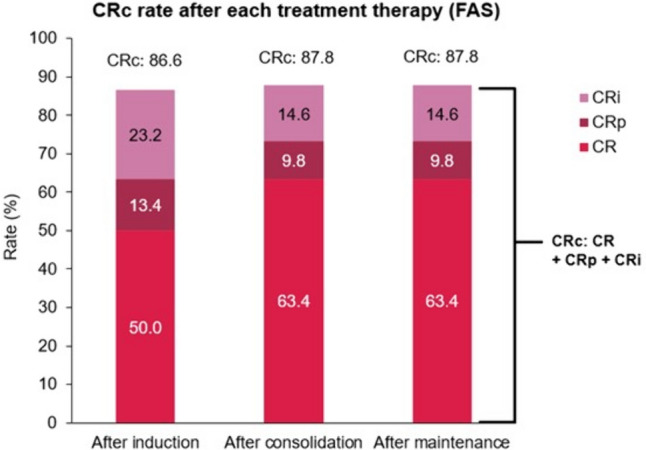
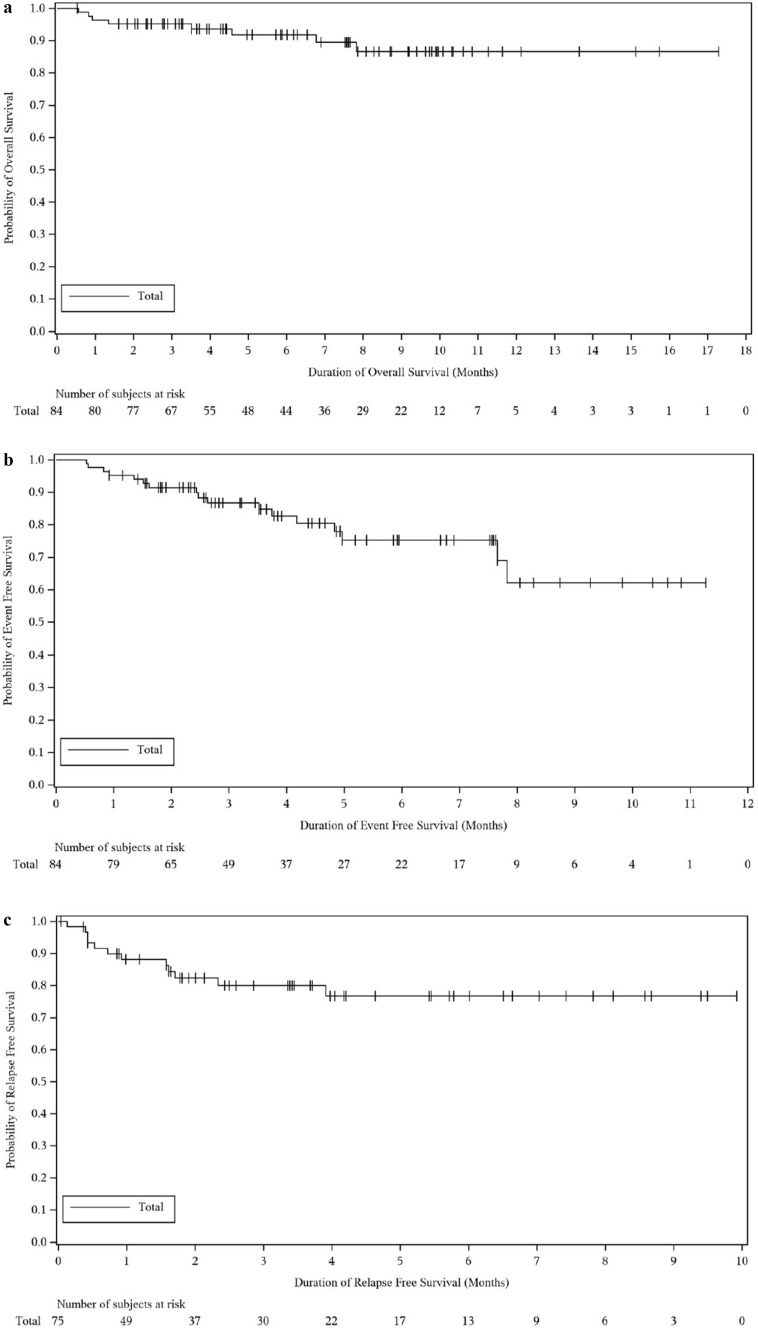
Results: In phase 1, MTD was not reached and RED was 120 mg/day. In phase 2, the CR rate was 50.0% after induction (90% confidence interval [CI] 40.4, 59.6); however, the lower confidence limit did not exceed the pre-defined 55% benchmark. Composite CR (CRc) rates were high following induction (86.6%, 95% CI [77.3, 93.1]), consolidation, and maintenance therapy (87.8%, 95% CI [78.7, 94.0], each). The probability of OS was 86.6% at 12 months. No new safety findings were reported.
Conclusion: In this interim analysis, gilteritinib 120 mg/day in combination with chemotherapy was well tolerated, with similar CRc rates to previous studies.
Keywords: FLT3 mutation; Acute myeloid leukemia; Chemotherapy; Gilteritinib; Newly diagnosed.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Sawa M reports payment/honoraria from Janssen Pharma and Sanofi. Miyamoto T reports payment/honoraria from Takeda Pharmaceutical Co., Otsuka Pharmaceutical Co., Ltd., MSD Co., Ltd, Astellas Pharmaceutical Co., Ltd., Janssen Co., Ltd., Abbvie Pharmaceutical Co., Ltd., and Kyowa Kirin Pharmaceutical Co. Kim H-J reports consulting fees from Astellas and honoraria from Astellas, and participated in advisory boards for Astellas. Cheong J-W reports payment/honoraria from Astellas, Bristol Myers Squibb, Merck, and GSK, and acted in a leadership/fiduciary role for The Korean Society of Hematology, AML/MDS Working Party, and The Korean Society of Blood and Marrow Transplantation. Naoe T reports payment/honoraria from Bristol Myers Squibb, Pfizer, Nippon Shinyaku, Astellas, Otsuka Pharma, and Japan Tissue Engineering. Akashi K reports grants from Asahi Kasei Pharma, Chugai Pharmaceutical, Kyowa Kirin and Sumitomo Pharma, and payment and/or honoraria from Asahi Kasei Pharma, Astellas, AstraZeneca, Abbvie, Kyowa Kirin, Chugai Pharmaceutical, Bristol Myers Squibb and Janssen Pharmaceuticals. Hill J reports stocks with Ligacept, LLC and is an employee of Astellas Pharma Inc. Kosako M, Ikegaya M, Terada W, Kadokura T, Gill SC, Heinloth A and Hasabou N are employees of Astellas Pharma Inc. Ikezoe T is editor of International Journal of Hematology. Hiramatsu Y, Morita S, and Miyawaki S have no disclosures to report.
Figures
References
-
- Lubeck DP, Danese M, Jennifer D, Miller K, Richhariya A, Garfin PM. Systematic literature review of the global incidence and prevalence of myelodysplastic syndrome and acute myeloid leukemia. Blood. 2016;128:5930–5930.
-
- U.S. Department of Health and Human Services. SEER Cancer Stat Facts: AML [Internet]. [cited 2023 Dec 7]. Available from: https://seer.cancer.gov/statfacts/html/amyl.html
-
- Canadian Cancer Statistics Advisory Commitee. Canadian Cancer Statistics. [Internet]. 2019. Available from: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2019-stat...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
