

Methylphenidate and Atomoxetine in Pregnancy and Possible Adverse Fetal Outcomes: A Systematic Review and Meta-Analysis
- PMID: 39504019
- PMCID: PMC11541644
- DOI: 10.1001/jamanetworkopen.2024.43648
Methylphenidate and Atomoxetine in Pregnancy and Possible Adverse Fetal Outcomes: A Systematic Review and Meta-Analysis
Erratum in
-
Error in Abstract, Results, and Figure.JAMA Netw Open. 2025 Apr 1;8(4):e2510141. doi: 10.1001/jamanetworkopen.2025.10141. JAMA Netw Open. 2025. PMID: 40198075 Free PMC article. No abstract available.
Abstract
Importance: Attention-deficit/hyperactivity disorder (ADHD) is one of the most common neurobehavioral disorders, and it afflicts about 7% of young people. As a consequence, many young women might be pregnant while taking medication for ADHD, but data about safety have not yet been strictly examined.
Objective: To examine adverse effects in offspring of mothers receiving treatment with atomoxetine and methylphenidate during pregnancy.
Data sources: Electronic databases (PubMed, Embase, and PsycINFO) were searched for articles published through December 31, 2023, with the following search terms: (atomoxetine OR methylphenidate) AND (pregnancy).
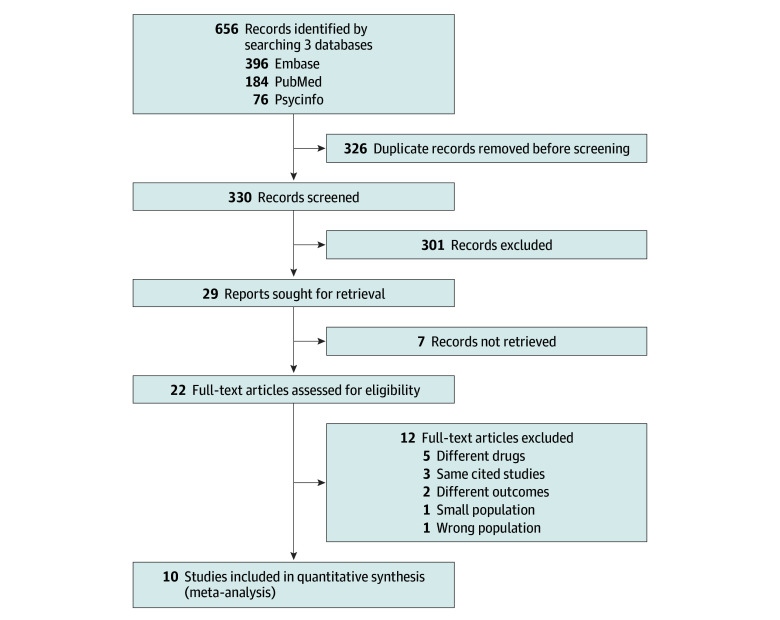
Study selection: Observational studies (eg, cohort studies, case-control studies, case-crossover studies, cross-sectional studies, and registry-based studies) that reported offspring outcomes in pregnancy with atomoxetine and/or methylphenidate and in mothers with ADHD but unexposed to ADHD treatment during pregnancy or from the general population were included. Ten studies of 656 records satisfied criteria.
Data extraction and synthesis: Two independent reviewers performed data extraction according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Meta-analyses were conducted based on reported odds ratios (ORs) and corresponding 95% CIs using a linear random effects model. Each study was inversely weighted by the reported variance of the estimators. Risk of publication bias and analysis of heterogeneity through univariate and multivariate metaregressions were also rated. Data were analyzed from January to March 2024.
Main outcomes and measures: Study outcomes included miscarriages and congenital anomalies.
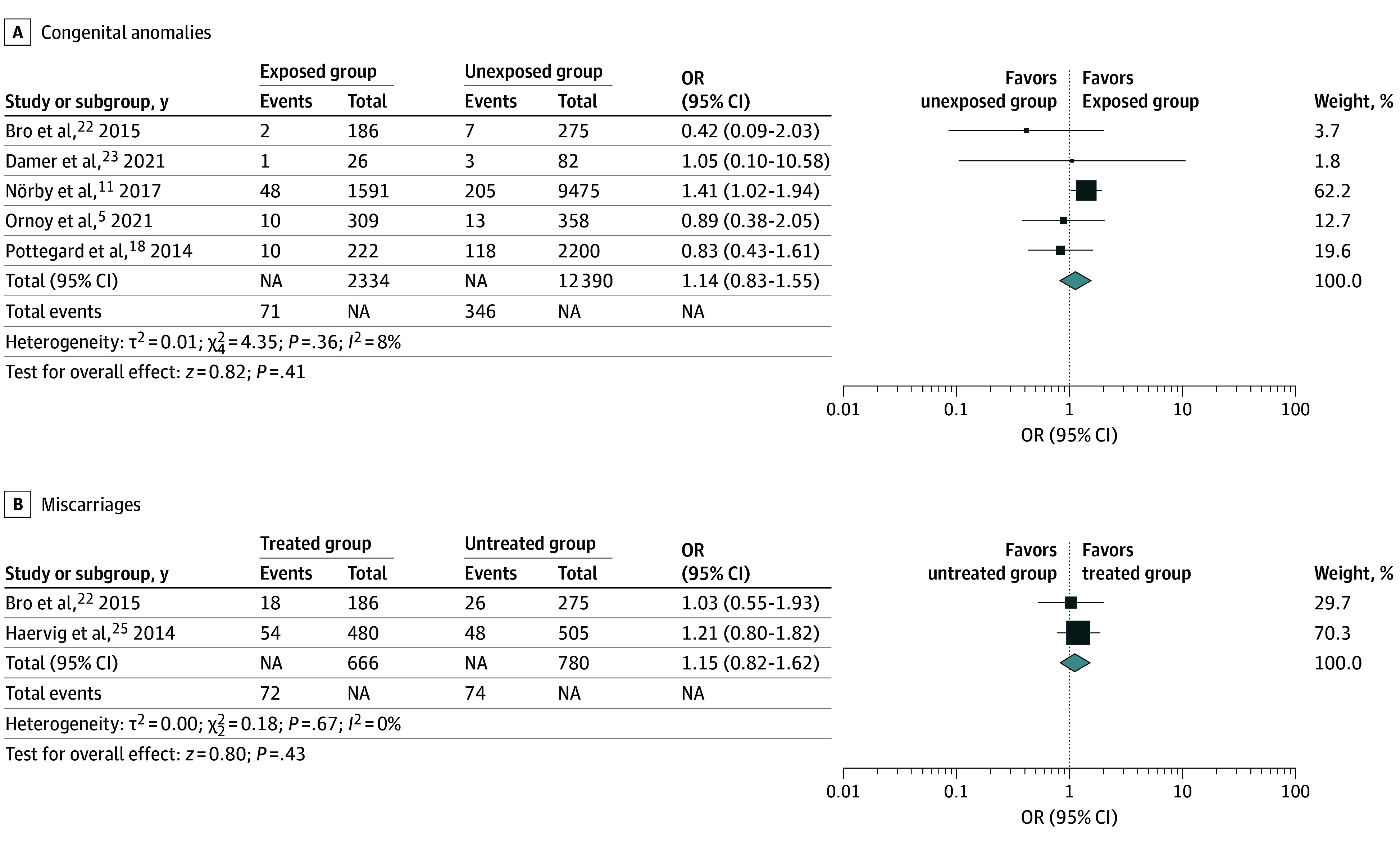
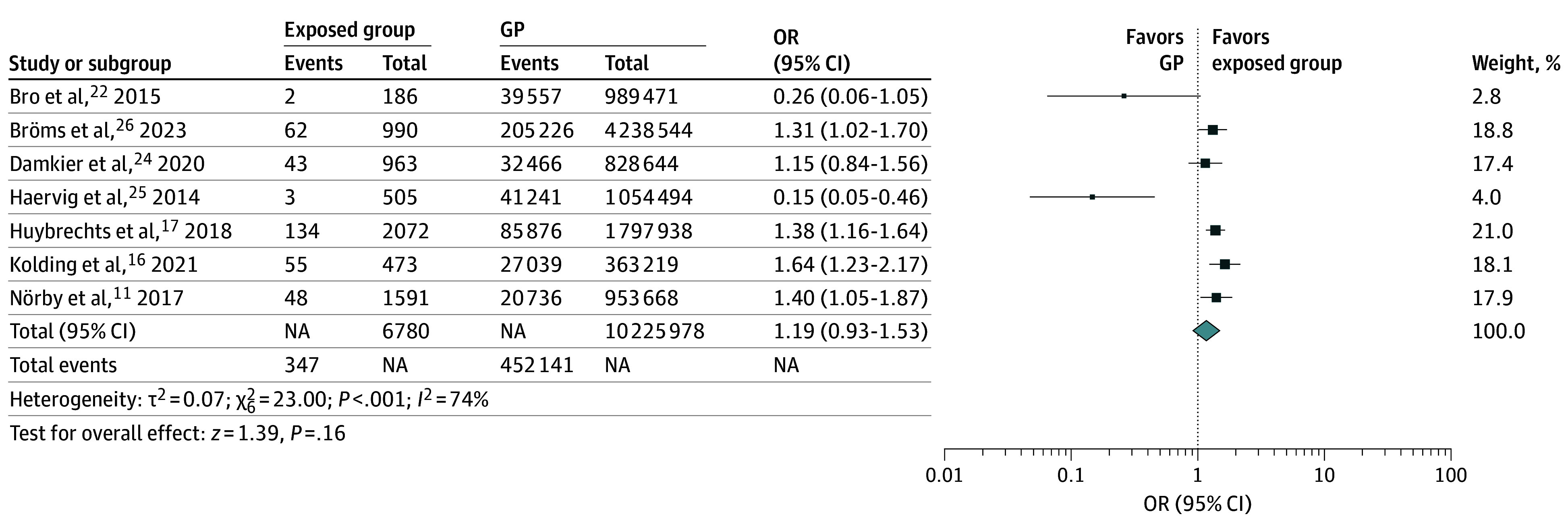
Results: Ten studies involving 16 621 481 pregnant women, 30 830 of them affected by ADHD, were included. Congenital anomalies or miscarriages were not more frequent in offspring of mothers receiving treatment with methylphenidate or atomoxetine during pregnancy compared with unexposed offspring (OR, 1.14; 95% CI, 0.83-1.55; P = .41; I2 = 8% for congenital anomalies; OR, 1.01; 95% CI, 0.70-1.47; P = .96; I2 = 0% for miscarriages) or compared with the general population (OR, 1.19; 95% CI, 0.93-1.53; P = .16; I2 = 74% for congenital anomalies; OR, 1.05, 95% CI, 0.81-1.37; P = .70; I2 = 0% for miscarriage).
Conclusions and relevance: Evidence from this meta-analysis, which involves a substantial sample of pregnant women with and without ADHD, suggests the maintenance of methylphenidate or atomoxetine during pregnancy is safe, given that congenital anomalies and miscarriages did not appear to significantly increase. Further studies are recommended to support and confirm these findings.
Conflict of interest statement
Figures

References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 4th ed. American Psychiatric Association; 1994.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
