

Influence of maternal hyperglycemia on placental capillary distribution
- PMID: 39504088
- PMCID: PMC11634342
- DOI: 10.31744/einstein_journal/2024AO0583
Influence of maternal hyperglycemia on placental capillary distribution
Abstract
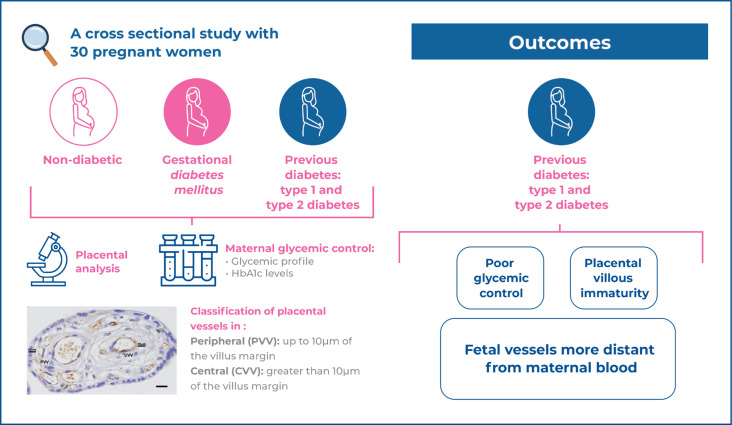
Objective: This study was conducted to investigate the distribution of placental villous vessels in pregnant women with different degrees of hyperglycemia.
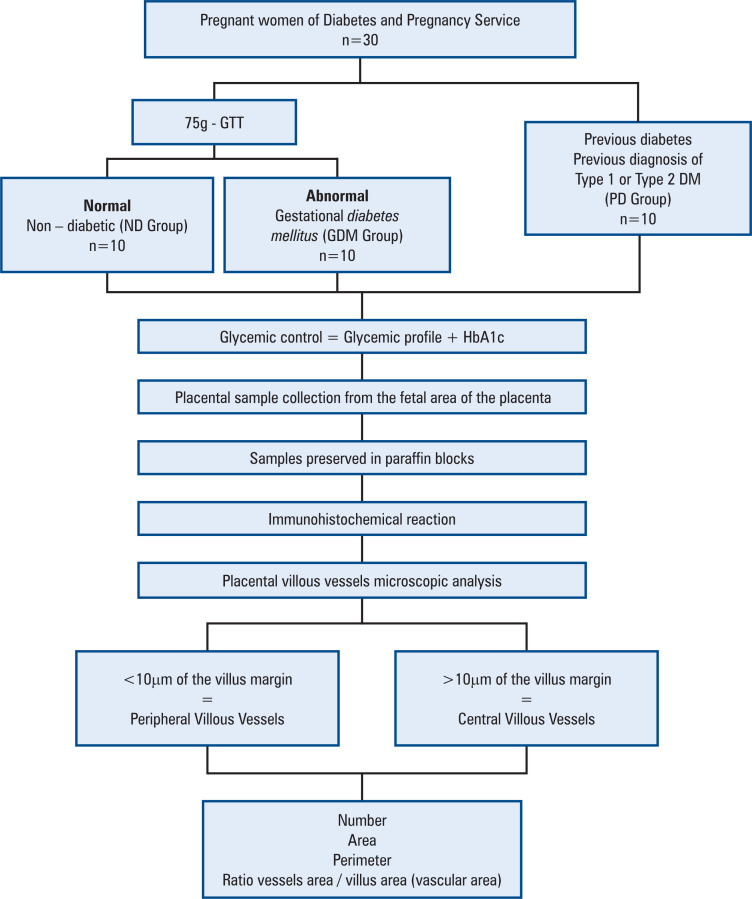
Methods: A cross-sectional study was performed using placental samples from 30 pregnant women without diabetes (n=10), with gestational diabetes mellitus (n=10), and with previous diabetes (type 1 and type 2 diabetes; n=10). Maternal glycemic control was evaluated using the glycemic mean and glycated hemoglobin levels. Placental samples were obtained during elective cesarean sections and processed for villous vessel analysis using immunohistochemistry for Von Willebrand factor. Vessels within 10μm of the villus margin were classified as peripheral, and vessels at a distance greater than 10μm were classified as central. The number, area, and perimeter of all vessels were evaluated, and the relationship between vessel area and total area of placental villus was calculated.
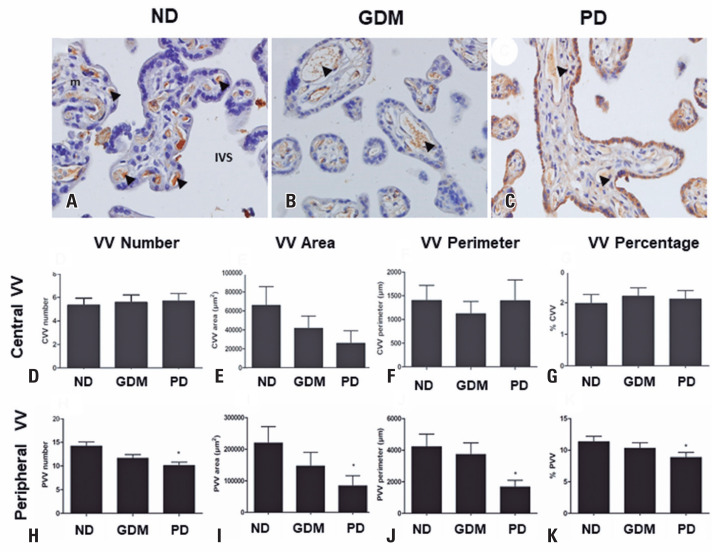
Results: Pregnant women with gestational diabetes mellitus and those with previous diabetes had higher glycated hemoglobin levels. The number of vessels was reduced in the villi of the previous Diabetes Group owing to peripheral reduction. Additionally, the area, perimeter, and percentage of peripheral blood were lower in the previous Diabetes Group than in the Non-Diabetic Group.
Conclusion: Maternal glycemic levels can modify placental capillary distribution.
Plain language summary
Moreli et al. demonstrated a reduction in vessels in the periphery of the placental villi in pregnant women with previous diabetes (type 1 and type 2). The placental vessels of this population are more distant from the maternal blood and may represent placental villous immaturity. These results were obtained when we classified the villous vessels as central or peripherial using 10μm of the villus margin as a reference.
Conflict of interest statement
Figures


References
-
- ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Hilliard ME, Isaacs D, Johnson EL, Kahan S, Khunti K, Leon J, Lyons SK, Perry ML, Prahalad P, Pratley RE, Seley JJ, Stanton RC, Gabbay RA. on behalf of the American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19–S40. Erratum in: Diabetes Care. 2023 Feb 01. Erratum in: Diabetes Care. 2023;46(9):1715. Review. - PMC - PubMed
-
- Reece EA. The fetal and maternal consequences of gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2010;23(3):199–203. Review. - PubMed
-
- Desoye G, Hauguel-de Mouzon S. The human placenta in gestational diabetes mellitus. The insulin and cytokine network. Diabetes Care. 2007;30(Suppl 2):S120–S126. Erratum in: Diabetes Care. 2007;30(12):3154. Review. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
