

Evaluation of the Vaginal Panel Realtime PCR kit (Vircell, SL) for diagnosing vaginitis: A comparative study with routinely used diagnostics
- PMID: 39504318
- PMCID: PMC11540222
- DOI: 10.1371/journal.pone.0313414
Evaluation of the Vaginal Panel Realtime PCR kit (Vircell, SL) for diagnosing vaginitis: A comparative study with routinely used diagnostics
Abstract
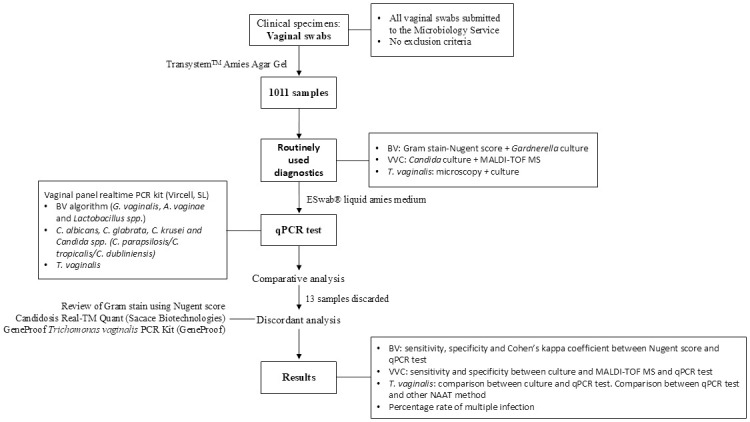
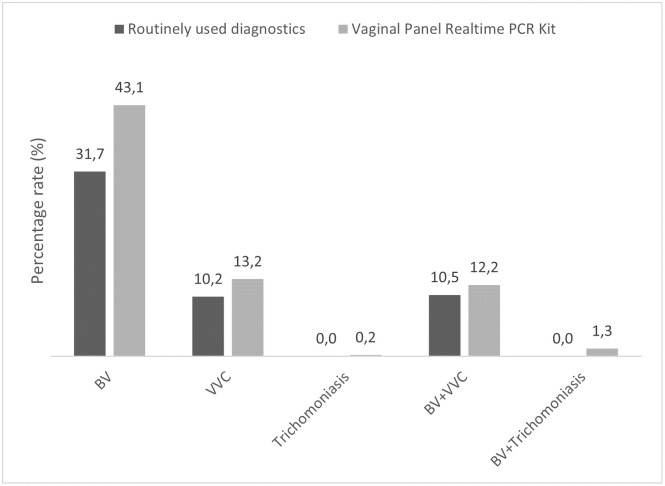
Vaginitis is a prevalent clinical disorder associated with several adverse health consequences, prompting women to seek medical care. In this study we evaluate the Vaginal Panel Real-Time PCR kit (qPCR test) against routinely used diagnostics for detection of bacterial vaginosis (BV), vulvovaginal candidiasis (VVC), and trichomoniasis. A total of 1011 vaginal swab specimens were analyzed. The routinely diagnostic methods for BV was Gram stain-based Nugent score. VVC presence was detected by culture, and Candida species were identified using MALDI-TOF MS. Trichomonas vaginalis was identified by culture in a selective medium. Molecular analyses were conducted on the MagXtract® 3200 System and analyzed using the CFX96™ Real-Time PCR Detection System. The sensitivity, specificity, positive predictive value, and negative predictive value of the qPCR test compared to the reference method for BV diagnosis was 93.1%, 88.8%, 90.1% and 92.2%, respectively, with a Kappa value of 0.82. For Candida species, sensitivity, specificity, positive predictive value, and negative predictive value were 96.0%, 98.4%, 95.3%, and 98.7%, respectively. The qPCR test detected 32 additional positive samples for Candida not reported by the routinely used diagnostics. For trichomoniasis, the qPCR test identified T. vaginalis in fifteen specimens, despite no microscopic detection in cultured specimens. Our results demonstrate that the Vaginal Panel Real-Time PCR kit shows optimal concordance with routinely used diagnostics for diagnosing vaginitis. Furthermore, enhancing detection of T. vaginalis. However, further validation studies are necessary to confirm its full diagnostic accuracy. The use of nucleic acid amplification tests (NAATs) provides rapid and accurate diagnosis, crucial for early detection and treatment of vaginitis.
Copyright: © 2024 Amor et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The funder provided support in the form of salaries for authors IA, SUP and PM, but did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The specific roles of these authors are articulated in the ‘author contributions’ section. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Paladine HL, Desai UA. Vaginitis: Diagnosis and Treatment. Am Fam Physician. 2018;97: 321–329. Available: http://www.aafp.org/afp/2018/0301/p321-s1.html. - PubMed
-
- Eckert LO. Acute Vulvovaginitis. New England Journal of Medicine. 2006;355: 1244–1252. - PubMed
-
- Cancelo Hidalgo MJ, Beltrán Vaquero D, Calaf Alsina J, Campillo Arias-Camisón F, Cano Sánchez A, Guerra Guirao JA, et al.. The protocol of the Spanish Society of Obstetrics and Gynecology for the diagnosis and treatment of vulvovaginal infection. Update 2012. Progresos de Obstetricia y Ginecologia. 2013;56: 278–284. doi: 10.1016/j.pog.2012.09.006 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
