

Remote Patient Monitoring and Digital Therapeutics Enhancing the Continuum of Care in Heart Failure: Nonrandomized Pilot Study
- PMID: 39504548
- PMCID: PMC11579625
- DOI: 10.2196/53444
Remote Patient Monitoring and Digital Therapeutics Enhancing the Continuum of Care in Heart Failure: Nonrandomized Pilot Study
Abstract
Background: Heart failure (HF) is the primary cause of hospitalization among Canadian patients aged ≥65 years. Care for HF requires regular clinical follow-ups to prevent readmissions and facilitate medical therapy optimization. Multiple barriers lead to therapeutic medical inertia including limited human resources and regional inequities. Remote patient monitoring (RPM) and digital therapeutics (DTx) solutions have been developed to improve HF management, but their adoption remains limited and underexplored. The Continuum project emerged as a collaborative initiative involving a health care center, a software start-up, and an industrial partner.
Objective: We aimed to develop and test the feasibility of the Continuum intervention that seamlessly combined an RPM system with a DTx solution for HF within the same software.
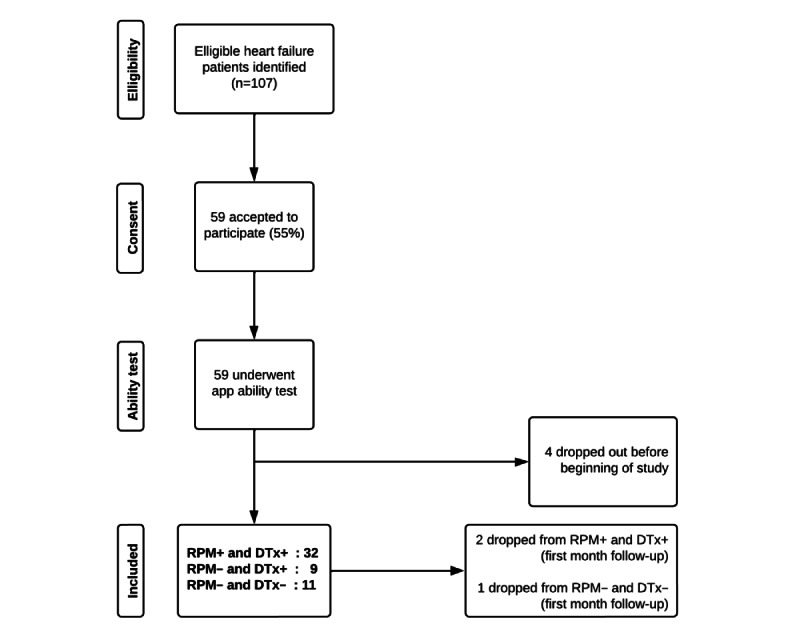
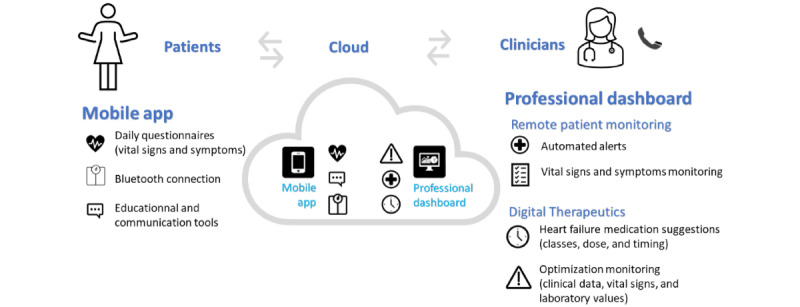
Methods: A 3-month pre-post pilot study was conducted from October 2020 to June 2021. Patients with HF who owned a smartphone or tablet (having remote patient monitoring [RPM+]), had (1) access to a self-care app where they could enter their vital signs, weight, and HF symptoms and view educational content; (2) daily monitoring of their data by a nurse; and (3) a DTx module with automated HF medication suggestions based on national guidelines, made available to their treating medical team. Bluetooth devices were offered to facilitate data recording. Nurses on RPM monitoring could call patients and arrange appointments with their medical team. Patients without a mobile device or unable to use the app were followed in another group (without remote patient monitoring [RPM-]).
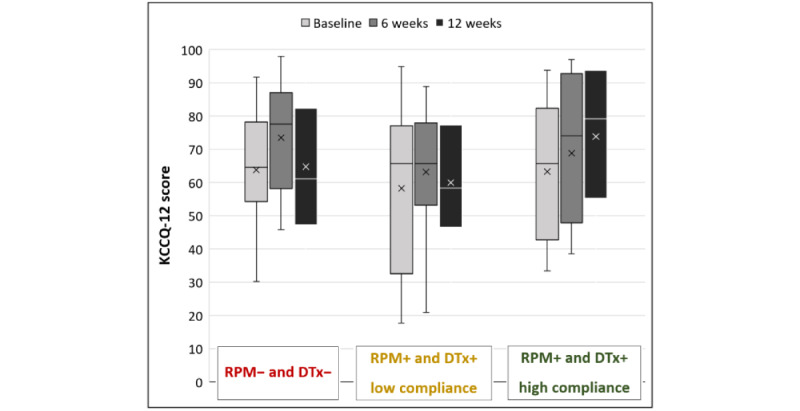
Results: In total, 52 patients were enrolled in this study (32 RPM+ and 20 RPM-). Among patients owning a mobile device, only 14% (5/37) could not use the app. In the RPM+ group, 47% (15/32) of the patients used the app for more than 80% (67 days) of the 12-week study period. The use of our digital solution was integrated into the regular nursing workday and only 34 calls had to be made by the nurse during the study period. Only 6% (2/32) of the patients in the RPM+ group experienced at least 1 all-cause hospitalization versus 35% (7/20) of the RPM- ones during the follow-up (6%, 2/32 vs 25%, 5/20 for HF hospitalization) and patients were more likely to have their HF therapy optimized if the DTx solution was available. Quality of life improved in patients compliant with the use of the mobile app (mean score variation +10.6, SD 14.7).
Conclusions: This pilot study demonstrated the feasibility of implementing our digital solution, within the specific context of HF. The seamless integration of Continuum into nursing workflow, mobile app accessibility, and adoption by patients, were the 3 main key learning points of this study. Further investigation is required to assess the potential impacts on hospitalizations, drug optimization, and quality of life.
Trial registration: ClinicalTrials.gov NCT05377190; https://clinicaltrials.gov/study/NCT05377190 (pilot study #21.403).
Keywords: digital health; digital therapeutics; heart; heart failure; medical therapy; medication optimization; mobile phone; patient care; pilot study; quality of life; remote patient management; symptoms; telemonitoring; therapeutics; vitals; weight.
©Emmanuel Marier-Tétrault, Emmanuel Bebawi, Stéphanie Béchard, Philippe Brouillard, Priccila Zuchinali, Emilie Remillard, Zoé Carrier, Loyda Jean-Charles, John Nam Kha Nguyen, Pascale Lehoux, Marie-Pascale Pomey, Paula A B Ribeiro, François Tournoux. Originally published in JMIR Formative Research (https://formative.jmir.org), 06.11.2024.
Conflict of interest statement
Conflicts of Interest: EM-T and FT have received speaker fees from Boehringer Ingelheim Canada, and both are board members of the Quebec Heart Failure Society. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this paper.
Figures


References
-
- Hospital stays in Canada. Canadian Institute for Health Information; 2023. [2024-08-26]. https://www.cihi.ca/en/hospital-stays-in- canada .
-
- McDonald M, Virani S, Chan M, Ducharme A, Ezekowitz JA, Giannetti N, Heckman GA, Howlett JG, Koshman SL, Lepage S, Mielniczuk L, Moe GW, O'Meara E, Swiggum E, Toma M, Zieroth S, Anderson K, Bray SA, Clarke B, Cohen-Solal A, D'Astous M, Davis M, De S, Grant ADM, Grzeslo A, Heshka J, Keen S, Kouz S, Lee D, Masoudi FA, McKelvie R, Parent M, Poon S, Rajda M, Sharma A, Siatecki K, Storm K, Sussex B, Van Spall H, Yip AMC. CCS/CHFS heart failure guidelines update: defining a new pharmacologic standard of care for heart failure with reduced ejection fraction. Can J Cardiol. 2021;37(4):531–546. doi: 10.1016/j.cjca.2021.01.017.S0828-282X(21)00055-6 - DOI - PubMed
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A, ESC Scientific Document Group 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi: 10.1093/eurheartj/ehab368. https://hdl.handle.net/2268/290864 6358045 - DOI - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2022;145(18):e895–e1032. doi: 10.1161/CIR.0000000000001063. https://www.ahajournals.org/doi/abs/10.1161/CIR.0000000000001063?url_ver... - DOI - PubMed
-
- Jarjour M, Henri C, de Denus S, Fortier A, Bouabdallaoui N, Nigam A, O'Meara E, Ahnadi C, White M, Garceau P, Racine N, Parent M, Liszkowski M, Giraldeau G, Rouleau J, Ducharme A. Care gaps in adherence to heart failure guidelines: clinical inertia or physiological limitations? JACC Heart Fail. 2020;8(9):725–738. doi: 10.1016/j.jchf.2020.04.019. https://linkinghub.elsevier.com/retrieve/pii/S2213-1779(20)30333-4 S2213-1779(20)30333-4 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
