

Mosaic chromosomal alterations (mCAs) in individuals with monoclonal B-cell lymphocytosis (MBL)
- PMID: 39505849
- PMCID: PMC11541990
- DOI: 10.1038/s41408-024-01175-8
Mosaic chromosomal alterations (mCAs) in individuals with monoclonal B-cell lymphocytosis (MBL)
Abstract
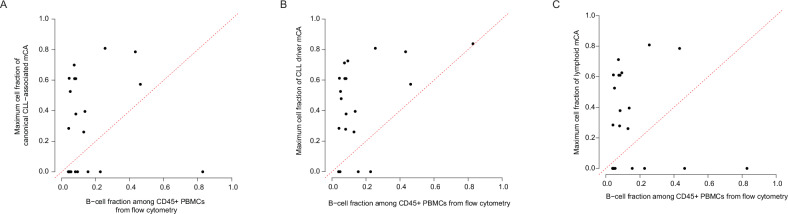
MBL is a precursor condition to chronic lymphocytic leukemia (CLL), characterized by monoclonal B-cells in blood. Mosaic chromosomal alterations (mCAs) are a form of clonal hematopoiesis that include gains, losses, and copy-neutral loss-of-heterozygosity of large DNA segments. Both MBL and mCAs have been found to increase the risk of CLL and lymphoid malignancies, and the aim of our study was to investigate how mCAs relate to MBL, which is currently unknown. We analyzed genetic, flow cytometric, and hematologic data from 4632 individuals from the Mayo Clinic Biobank and CLL Database. MBL was detected using flow cytometry and classified as high-count (HC) or low-count (LC) MBL based on clone size. mCAs were detected primarily from whole blood DNA using sensitive SNP-array-based analyses. mCAs commonly altered in CLL (deletion of 6q, 11q, 13q, 17p, and trisomy 12) were specific (>99%) to individuals with MBL and CLL. HC-MBL and LC-MBL individuals were 881-fold and 8-fold, respectively, more likely to harbor CLL-associated mCAs than those without MBL. The cell fraction bearing these mCAs typically exceeded the B-cell fraction, suggesting their origin prior to the B-cell lineage. Integrating genetic and blood count data enabled detecting HC-MBL with high specificity in a biobank sample. These results quantify the contribution of mCAs to MBL and could enable large studies of HC-MBL without the need for flow cytometric screening.
© 2024. The Author(s).
Conflict of interest statement
AS stock in Vertex Pharmaceuticals and consulting for Alight. SAP Research funding has been provided to the institution from Janssen, AstraZeneca, Merck, and Genentech for clinical studies in which Sameer A. Parikh is a principal investigator. Honoraria has been provided to the institution from Pharmacyclics, Merck, AstraZeneca, Janssen, Genentech, Amgen, MingSight Pharmaceuticals, TG Therapeutics, Eli Lilly, Novalgen Limited, Kite Pharma, and AbbVie for Sameer A. Parikh’s participation in consulting activities/advisory board meetings. PJH: None. NEK: Advisory Board for AbbVie, AstraZeneca, Beigene, Behring, Boehringer Ingelheim Pharmaceuticals, Inc., Dava Oncology, Janssen, Juno Therapeutics, Pharmacyclics. DSMC (Data Safety Monitoring Committee) for Agios Pharm, AstraZeneca, BMS –Celgene, Dren Bio Janssen. Research funding from: AbbVie, Acerta Pharma, Bristol Meyer Squib, Celgene, Genentech, Pharmacyclics, Sunesis, Vincerx. BLE: research funding from Celgene, Deerfield, Novartis, and Calico and consulting fees from Abbvie and GRAIL. He is a member of the scientific advisory board and shareholder for Neomorph Inc., TenSixteen Bio, Skyhawk Therapeutics, and Exo Therapeutics.
Figures



References
Publication types
MeSH terms
Grants and funding
- R01CA235026/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
- R01 CA235026/CA/NCI NIH HHS/United States
- T32 CA009172/CA/NCI NIH HHS/United States
- R21CA282702/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
- K00 CA234943/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
