

A PSA SNP associates with cellular function and clinical outcome in men with prostate cancer
- PMID: 39505858
- PMCID: PMC11541583
- DOI: 10.1038/s41467-024-52472-6
A PSA SNP associates with cellular function and clinical outcome in men with prostate cancer
Abstract
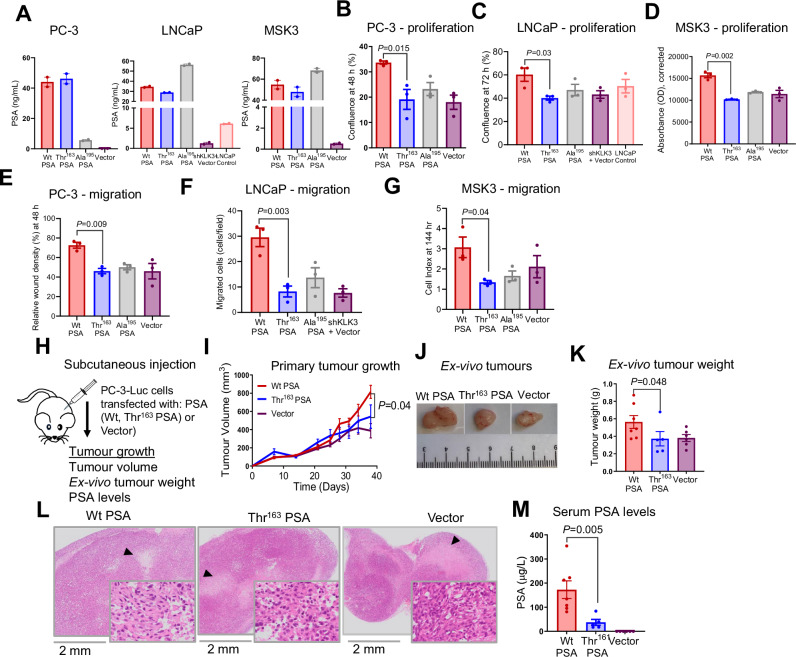
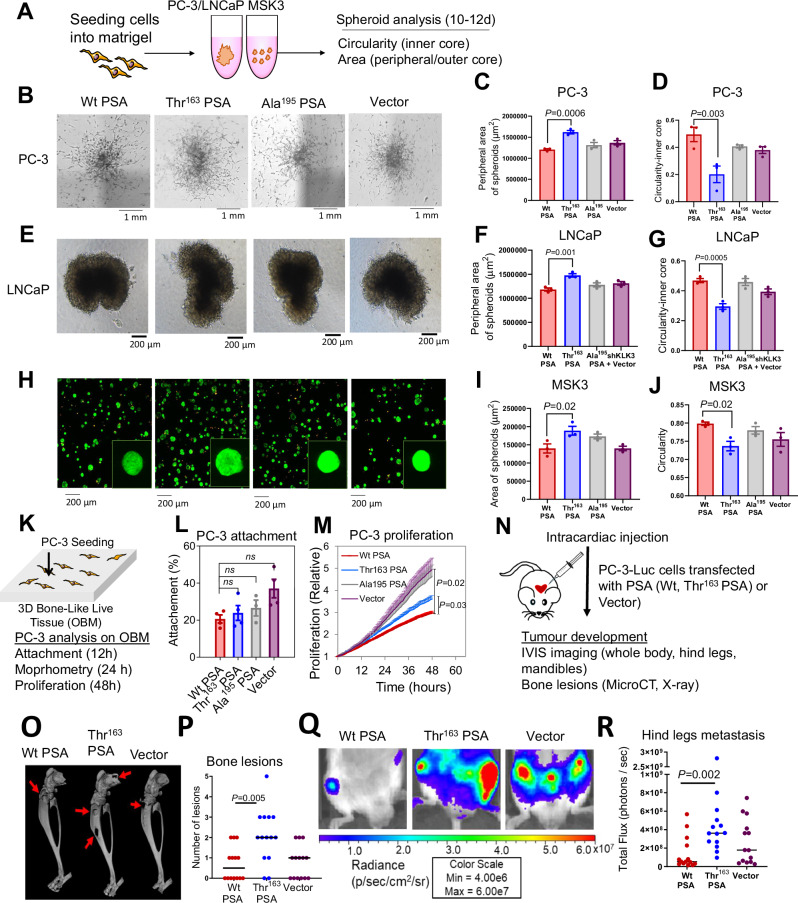
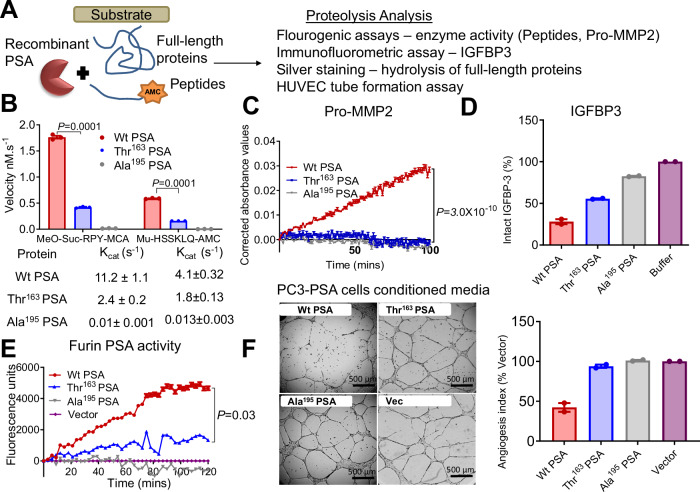
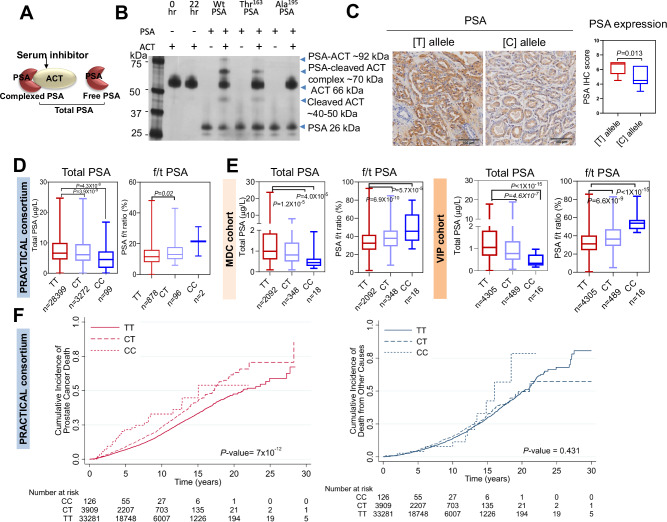
Genetic variation at the 19q13.3 KLK locus is linked with prostate cancer susceptibility in men. The non-synonymous KLK3 single nucleotide polymorphism (SNP), rs17632542 (c.536 T > C; Ile163Thr-substitution in PSA) is associated with reduced prostate cancer risk, however, the functional relevance is unknown. Here, we identify that the SNP variant-induced change in PSA biochemical activity mediates prostate cancer pathogenesis. The 'Thr' PSA variant leads to small subcutaneous tumours, supporting reduced prostate cancer risk. However, 'Thr' PSA also displays higher metastatic potential with pronounced osteolytic activity in an experimental metastasis in-vivo model. Biochemical characterisation of this PSA variant demonstrates markedly reduced proteolytic activity that correlates with differences in in-vivo tumour burden. The SNP is associated with increased risk for aggressive disease and prostate cancer-specific mortality in three independent cohorts, highlighting its critical function in mediating metastasis. Carriers of this SNP allele have reduced serum total PSA and a higher free/total PSA ratio that could contribute to late biopsy decisions and delay in diagnosis. Our results provide a molecular explanation for the prominent 19q13.3 KLK locus, rs17632542 SNP, association with a spectrum of prostate cancer clinical outcomes.
© 2024. The Author(s).
Conflict of interest statement
The patents mentioned herewith are not directly related to this study. H.L. is named on a patent for a statistical method to detect prostate cancer. The patent for the statistical model has been licensed and commercialised as the 4Kscore by OPKO Diagnostics. H.L. receives royalties from sales of this test and owns stock in OPKO. H.L. serves on SAB for Fujirebio Diagnostics. R.E. has the following conflicts of interest to declare: Honoraria from GU-ASCO, Janssen, University of Chicago, Dana Farber Cancer Institute USA as a speaker. Educational honorarium from Bayer and Ipsen, member of external expert committee to Astra Zeneca UK and Member of Active Surveillance Movember Committee. She is a member of the SAB of Our Future Health. She undertakes private practice as a sole trader at The Royal Marsden NHS Foundation Trust and 90 Sloane Street SW1X 9PQ and 280 Kings Road SW3 4NX, London, UK. All the other authors declare no conflict of interest.
Figures
Update of
-
Biochemical activity induced by a germline variation in KLK3 (PSA) associates with cellular function and clinical outcome in prostate cancer.Res Sq [Preprint]. 2023 Mar 28:rs.3.rs-2650312. doi: 10.21203/rs.3.rs-2650312/v1. Res Sq. 2023. Update in: Nat Commun. 2024 Nov 6;15(1):9587. doi: 10.1038/s41467-024-52472-6. PMID: 37034758 Free PMC article. Updated. Preprint.
References
-
- Carter, H. B. Prostate-Specific Antigen (PSA) Screening for Prostate Cancer: Revisiting the Evidence. JAMA319, 1866–1868 (2018). - PubMed
-
- de Vos, I. I. et al. A Detailed Evaluation of the Effect of Prostate-specific Antigen-based Screening on Morbidity and Mortality of Prostate Cancer: 21-year Follow-up Results of the Rotterdam Section of the European Randomised Study of Screening for Prostate Cancer. Eur. Urol.84, 426–434 (2023). - PubMed
-
- Kovac, E. et al. Association of Baseline Prostate-Specific Antigen Level With Long-term Diagnosis of Clinically Significant Prostate Cancer Among Patients Aged 55 to 60 Years A Secondary Analysis of a Cohort in the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. Jama Netw. Open3, e1919284 (2020). - PMC - PubMed
-
- Catalona, W. J. et al. Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial. JAMA279, 1542–1547 (1998). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
