

Measurable residual mutated IDH1 before allogeneic transplant for acute myeloid leukemia
- PMID: 39506075
- PMCID: PMC11810766
- DOI: 10.1038/s41409-024-02447-4
Measurable residual mutated IDH1 before allogeneic transplant for acute myeloid leukemia
Abstract
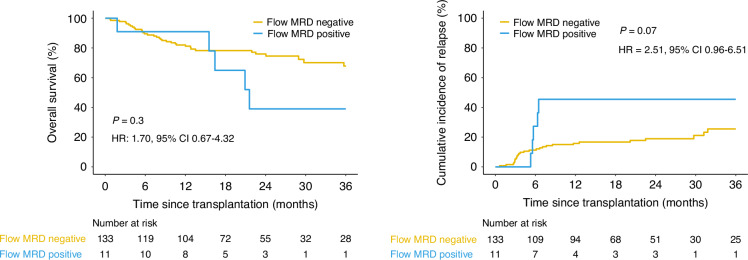
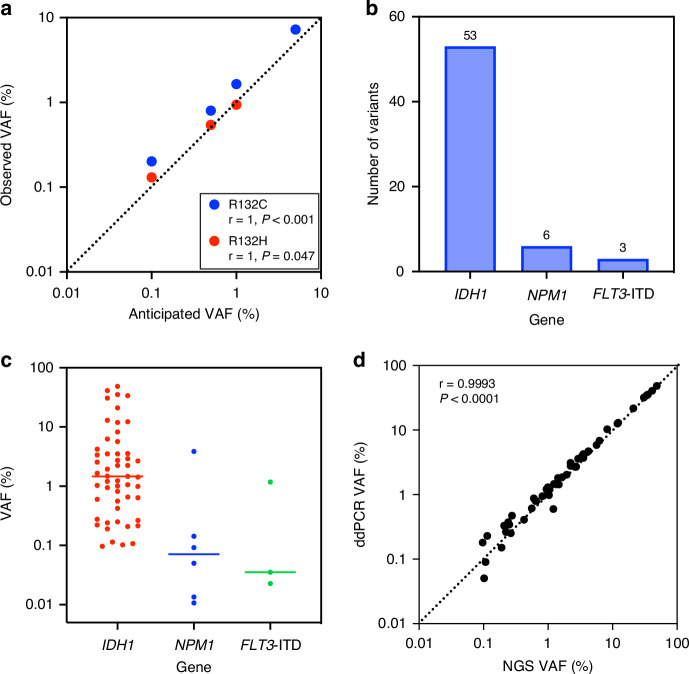
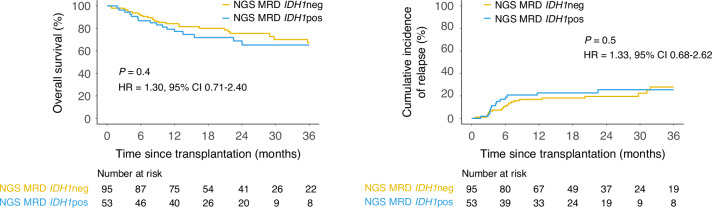
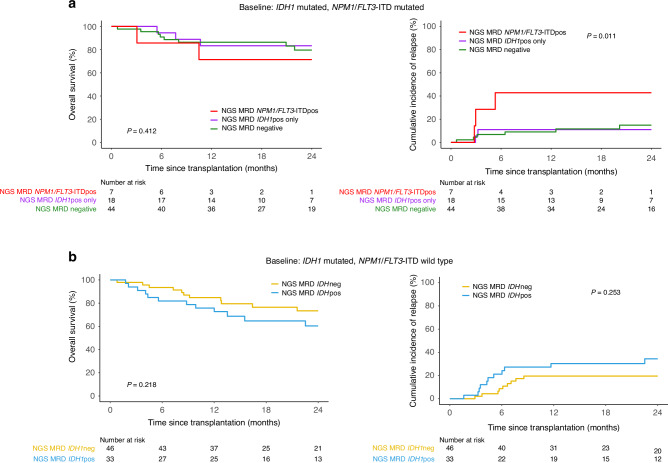
Measurable residual disease (MRD) in adults with acute myeloid leukemia (AML) in complete remission is an important prognostic marker, but detection methodology requires optimization. Persistence of mutated NPM1 or FLT3-ITD in the blood of adult patients with AML in first complete remission (CR1) prior to allogeneic hematopoietic cell transplant (alloHCT) associates with increased relapse and death after transplant. The prognostic implications of persistence of other common AML-associated mutations, such as IDH1, at this treatment landmark however remain incompletely defined. We performed testing for residual IDH1 variants (IDH1m) in pre-transplant CR1 blood of 148 adult patients undergoing alloHCT for IDH1-mutated AML at a CIBMTR reporting site between 2013 and 2019. No statistically significant post-transplant differences were observed between those testing IDH1m positive (n = 53, 36%) and negative pre-transplant (overall survival (OS): p = 0.4; relapse: p = 0.5). For patients with IDH1 mutated AML co-mutated with NPM1 and/or FLT3-ITD, only detection of persistent mutated NPM1 and/or FLT3-ITD was associated with significantly higher rates of relapse (p = 0.01). These data, from the largest study to date, do not support the detection of IDH1 mutation in CR1 blood prior to alloHCT as evidence of AML MRD for increased post-transplant relapse risk.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Competing interests: CSH: The National Heart, Lung, and Blood Institute receives research funding for the laboratory of CSH from the Foundation of the NIH AML MRD Biomarkers Consortium. JJA: Advisory Committee: AscellaHealth and Takeda. FEC: Consultant: SPD Oncology, Amgen, Association of Community Cancer Centers; Clinical Trial Grant Support (PI) to the University of Virginia: Amgen, BMS, Celgene, SPD Oncology, Sanofi, Bristol Myers Squibb, FibroGen, PharmaEssentia, BioSight, MEI Pharma, Novartis, Arog pharmaceuticals; Travel grant: DAVA Oncology. ECC: Consultant: Rigel Pharmaceuticals and AbbVie. YBC: Consultant: Incyte, Takeda, Astellas, Editas, Novo Nordisk, Pharmacosmos, Vor. AC: Employment: Bio-Rad Laboratories. AMJJ: Funding: Abbvie. MJGDL: Advisory Board: Pfizer, Bristol Myers Squibb; Data Safety Monitoring Board: Novartis, Abbvie; Research Funding: Miltenyi Biotec. MRL: Research support: Abbvie, Astellas, Amgen, Actinium, Pluristem, Sanofi; Speakers Bureau: Beigene, Amgen; Data Safety Monitoring Committee: Biosight. PK: Consultant: Pfizer, Jazz Pharmaceuticals Ethics approval and consent to participate: Protected health information for research was collected and maintained in CIBMTR’s capacity as a public health authority under the Health Insurance Portability and Accountability Act (HIPAA) privacy rule. All patients provided written informed consent for participation in the National Marrow Donor Program institutional review board–approved CIBMTR database (NCT01166009) and repository (NCT04920474) research protocols. Research was performed in compliance with all applicable federal regulations pertaining to the protection of human research participants and with the approval of the CIBMTR observational research group.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
