

Clinical outcomes in patients in any phase of CML treated with ponatinib in France-Data from the TOPASE observational study
- PMID: 39506529
- PMCID: PMC11637719
- DOI: 10.1111/bjh.19819
Clinical outcomes in patients in any phase of CML treated with ponatinib in France-Data from the TOPASE observational study
Abstract
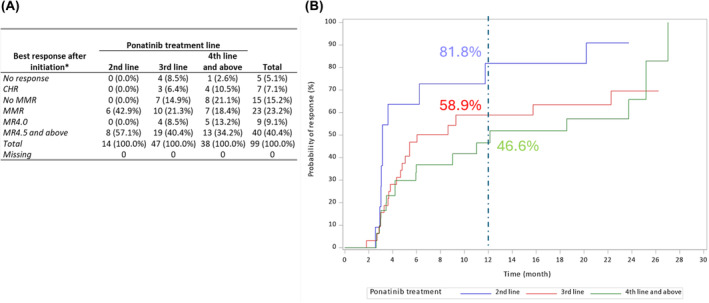
The TOPASE study was set up to evaluate the outcomes of chronic myeloid leukaemia [CML] patients treated with ponatinib (PON) in a real-world setting in France. One hundred and twenty CML patients, 105 in chronic phase (CP), 8 in accelerated phase (AP) and 7 in blastic phase (BP) were included. Fifty-one (49%) of the CP-CML patients were in third line of treatment. The trigger for PON initiation in CP-CML was 'poor response' in 67 patients, 'poor tolerance' in 28 patients and 'response enhancement' in seven patients. The median dose at initiation was 30 mg/day [Q1; Q3 = 15; 30] in CP-CML and 45 mg/day [Q1; Q3 = 30; 45] in AP/BP-CML. Of 98 CP-CML evaluable patients, 72 (73.5%) were considered as responders (MMR) at one time point at least once, especially for those in second line of treatment and/or presenting a T315I mutation. Ninety-six of 120 (80%) patients reported at least one adverse event. An arterial occlusive event (AOE) was reported in 11 patients (9.2%). Thus, these real-life data confirm the potency of ponatinib in resistant or intolerant patients with an acceptable safety profile in non-selected patients. NCT number: NCT04048564.
Keywords: CML; TKI; ponatinib; real‐life setting.
© 2024 The Author(s). British Journal of Haematology published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
FH is a consultant and speaker for Incyte Biosciences, Novartis, Pfizer. EC received honoraria from Novartis and Incyte. PCM is a speaker for Incyte. MH received grant from Incyte. VC is a board member and consultant for Incyte, Novartis and Pfizer. AMA is an employee of INCYTE France. AT is a consultant for Novartis, Bristol Myers Squibb and Abbvie. AT is also member of advisory Board for Novartis and is a speaker for Abbvie. FEN is an advisory board member for Novartis Pharma, Incyte Biosciences, Speaker for Incyte Biosciences, Novartis, Consultant for Novartis, Sun Pharma Ltd. FEN also received Institutional grants from Incyte Biosciences and Novartis. PR received research grant from Incyte. EM is a consultant for Incyte Biosciences, Novartis, Bayer and Pfizer. AGB, MGB, PR, VC, GE, AT and EC received financial support from Incyte to participate in the study's scientific committee. FH was specially commissioned to provide a critical review of the trial results. All other authors had no competing interest to disclose.
Figures

References
-
- Asciminib EMA authorisation and product characteristics information. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/scemblix
-
- Kantarjian HM, Giles FJ, Bhalla KN, Pinilla‐Ibarz J, Larson RA, Gattermann N, et al. Nilotinib is effective in patients with chronic myeloid leukemia in chronic phase after imatinib resistance or intolerance: 24‐month follow‐up results. Blood. 2011;117(4):1141–1145. 10.1182/blood-2010-03-277152 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
