

Risk factors for puncture-related complications after cerebrovascular angiography and neuroendovascular intervention with distal transradial approach
- PMID: 39506670
- PMCID: PMC11539764
- DOI: 10.1186/s12883-024-03940-5
Risk factors for puncture-related complications after cerebrovascular angiography and neuroendovascular intervention with distal transradial approach
Abstract
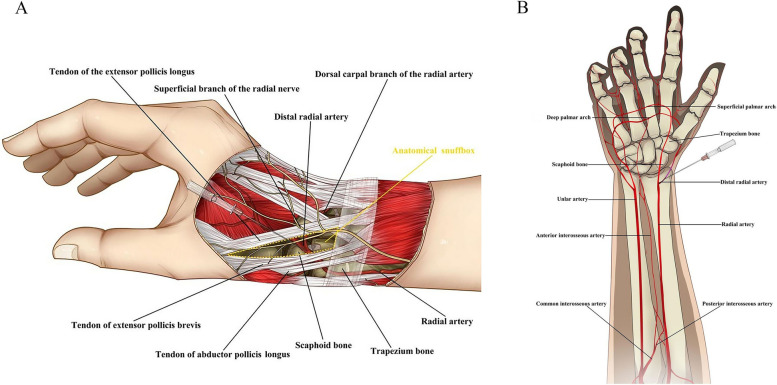
Background and purpose: To determine the risk factors for puncture-related complications after the distal transradial approach (dTRA) for cerebrovascular angiography and neuroendovascular intervention and to explore the incidence and potential mechanisms of procedural failure and puncture-related complications.
Materials and methods: From February to November 2023, 62 patients underwent dTRA in our department. Demographic, clinical, and procedural data were collected retrospectively. Postoperative puncture-related complications were defined as a syndrome of major hematoma, minor hematoma, arterial spasm/occlusion, arteriovenous fistula, pseudoaneurysm, and neuropathy. Univariate and multivariate logistic regressions were performed to identify significant factors contributing to puncture-related complications.
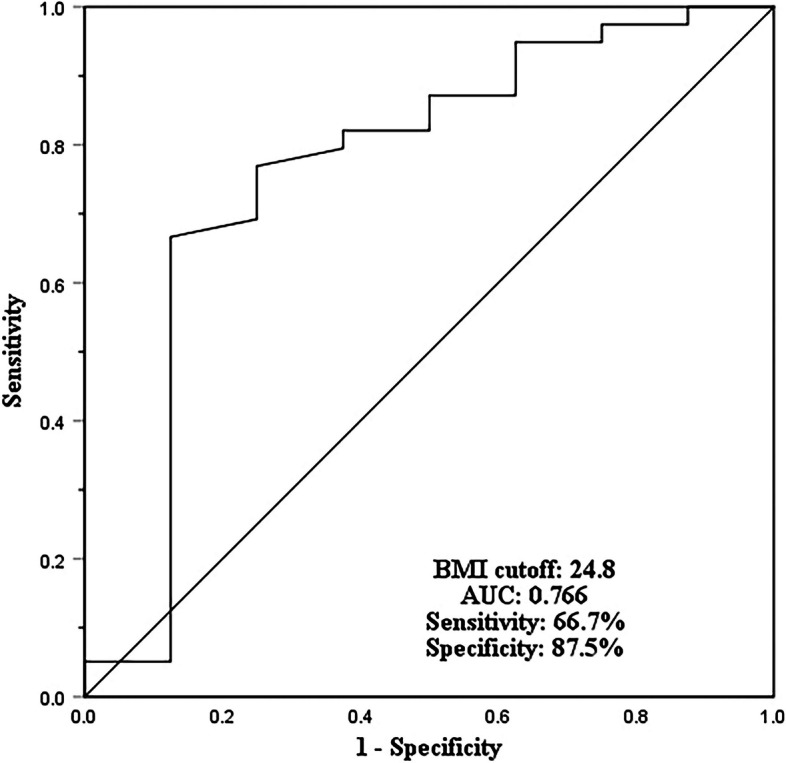
Results: Forty-five diagnostic cerebral angiograms and 17 neurointerventions were performed or attempted with dTRA in 62 patients. Procedural success was achieved via dTRA in 47 (75.8%) patients, whereas 15 (24.2%) required conversion to other approaches. Reasons for failure included puncture failure (n = 8), inability to cannulate due to arterial spasm (n = 6), and inadequate catheter support of the left vertebral artery (n = 1). 17.0% (8/47) of patients had postoperative puncture-related complications. Minor hematoma occurred in 8.5% (4/47) of patients, arterial spasm/occlusion in 6.3% (3/47), and neuropathy in 2.1% (1/47). No major complications were observed. On stepwise multivariable regression analysis, BMI (OR = 0.70, 95%CI 0.513 to 0.958; p = 0.026) was an independent risk factor for puncture-related complications, with a cut-off of 24.8 kg/m2 (sensitivity 66.7% and specificity 87.5%).
Conclusion: Our cohort is the first study of risk factors for puncture-related complications after neurointerventional interventions with dTRA. This study has shown that a low BMI (< 24.8 kg/m2) is independently associated with the development of puncture-related complications.
Keywords: Complications; Diagnostic cerebral angiography; Distal transradial approach; Risk factors.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Distal versus proximal transradial access for diagnostic cerebral angiography: A single-center experience.J Clin Neurosci. 2025 Jul;137:111283. doi: 10.1016/j.jocn.2025.111283. Epub 2025 May 6. J Clin Neurosci. 2025. PMID: 40334318 Clinical Trial.
-
Distal transradial access in the anatomical snuffbox for diagnostic cerebral angiography.J Neurointerv Surg. 2019 Jul;11(7):710-713. doi: 10.1136/neurintsurg-2019-014718. Epub 2019 Feb 27. J Neurointerv Surg. 2019. PMID: 30814329
-
Distal Transradial Artery Access for Neuroangiography and Neurointerventions : Pitfalls and Exploring the Boundaries.Clin Neuroradiol. 2022 Jun;32(2):427-434. doi: 10.1007/s00062-021-01039-9. Epub 2021 Jul 13. Clin Neuroradiol. 2022. PMID: 34258635 Free PMC article.
-
Transradial approach for neurointerventions: a systematic review of the literature.J Neurointerv Surg. 2020 Sep;12(9):886-892. doi: 10.1136/neurintsurg-2019-015764. Epub 2020 Mar 9. J Neurointerv Surg. 2020. PMID: 32152185 Free PMC article.
-
Transradial access for neurointerventions: management of access challenges and complications.J Neurointerv Surg. 2020 Jan;12(1):82-86. doi: 10.1136/neurintsurg-2019-015145. Epub 2019 Jul 26. J Neurointerv Surg. 2020. PMID: 31350370 Review.
Cited by
-
Massive Hemothorax Following Transradial Coronary Angioplasty.Cureus. 2025 Mar 7;17(3):e80236. doi: 10.7759/cureus.80236. eCollection 2025 Mar. Cureus. 2025. PMID: 40196101 Free PMC article.
References
-
- Sinha SK, Jha MJ, Mishra V, et al. Radial Artery Occlusion - Incidence, Predictors and Long-term outcome after TRAnsradial Catheterization: clinico-Doppler ultrasound-based study (RAIL-TRAC study). Acta Cardiol. 2017;72(3):318–27. - PubMed
-
- Sgueglia GA, Lee BK, Cho BR, et al. Distal Radial Access: Consensus Report of the First Korea-Europe Transradial Intervention Meeting. JACC Cardiovasc Interv. 2021;14(8):892–906. - PubMed
-
- Brunet MC, Chen SH, Sur S, et al. Distal transradial access in the anatomical snuffbox for diagnostic cerebral angiography. J Neurointerv Surg. 2019;11(7):710–3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
