

The role of heparan sulfate in enhancing the chemotherapeutic response in triple-negative breast cancer
- PMID: 39506780
- PMCID: PMC11539583
- DOI: 10.1186/s13058-024-01906-6
The role of heparan sulfate in enhancing the chemotherapeutic response in triple-negative breast cancer
Abstract
Background: Breast cancer, one of the most common forms of cancer, is associated with the highest cancer-related mortality among women worldwide. In comparison to other types of breast cancer, patients diagnosed with the triple-negative breast cancer (TNBC) subtype have the worst outcome because current therapies do not produce long-lasting responses. Hence, innovative therapies that produce persisting responses are a critical need. We previously discovered that hyperactivating purinergic receptors (P2RXs) by increasing extracellular adenosine triphosphate (eATP) concentrations enhances TNBC cell lines' response to chemotherapy. Heparan sulfate inhibits multiple extracellular ATPases, so it is a molecule of interest in this regard. In turn, heparanase degrades polysulfated polysaccharide heparan sulfate. Importantly, previous work suggests that breast cancer and other cancers express heparanase at high levels. Hence, as heparan sulfate can inhibit extracellular ATPases to facilitate eATP accumulation, it may intensify responses to chemotherapy. We postulated that heparanase inhibitors would exacerbate chemotherapy-induced decreases in TNBC cell viability by increasing heparan sulfate in the cellular microenvironment and hence, augmenting eATP.
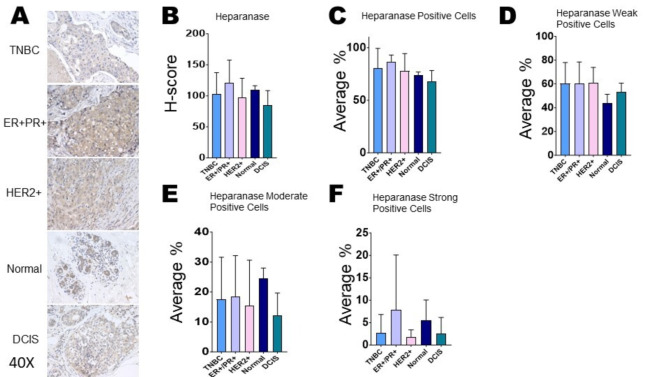
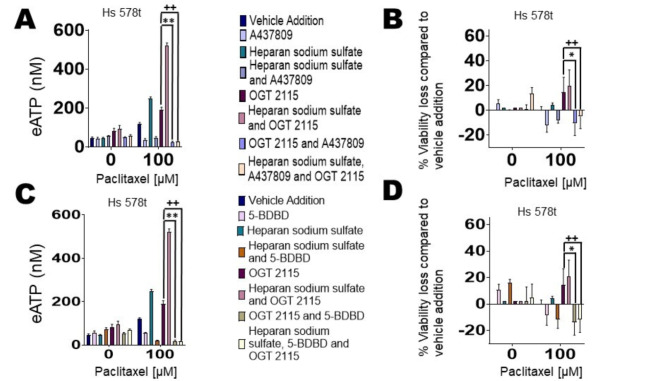
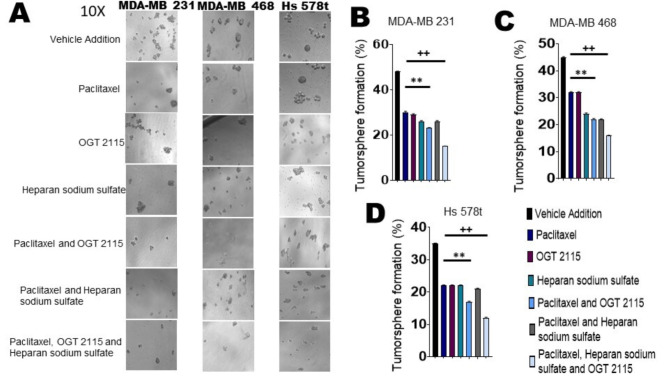
Methods: We treated TNBC cell lines MDA-MB 231, Hs 578t, and MDA-MB 468 and non-tumorigenic immortal mammary epithelial MCF-10A cells with paclitaxel (cytotoxic chemotherapeutic) with or without the heparanase inhibitor OGT 2115 and/or supplemental heparan sulfate. We evaluated cell viability and the release of eATP. Also, we compared the expression of heparanase protein in cell lines and tissues by immunoblot and immunohistochemistry, respectively. In addition, we examined breast-cancer-initiating cell populations using tumorsphere formation efficiency assays on treated cells.
Results: We found that combining heparanase inhibitor OGT 2115 with chemotherapy decreased TNBC cell viability and tumorsphere formation through increases in eATP and activation of purinergic receptors as compared to TNBC cells treated with single-agent paclitaxel.
Conclusion: Our data shows that by preventing heparan sulfate breakdown, heparanase inhibitors make TNBC cells more susceptible to chemotherapy by enhancing eATP concentrations.
Keywords: ATP; Breast cancer; Chemotherapy; Heparan sulfate; Heparanase; Purinergic signaling.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Update of
-
The role of heparan sulfate in enhancing the chemotherapeutic response in triple-negative breast cancer.bioRxiv [Preprint]. 2023 Sep 12:2023.09.08.556819. doi: 10.1101/2023.09.08.556819. bioRxiv. 2023. Update in: Breast Cancer Res. 2024 Nov 6;26(1):153. doi: 10.1186/s13058-024-01906-6. PMID: 37745355 Free PMC article. Updated. Preprint.
References
-
- Fisher CS, Ma CX, Gillanders WE, Aft RL, Eberlein TJ, Gao F, Margenthaler JA. Neoadjuvant chemotherapy is associated with improved survival compared with adjuvant chemotherapy in patients with triple-negative breast cancer only after complete pathologic response. Ann Surg Oncol. 2012;19(1):253–8. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
