

Impella 5.5 as a bridge-to-surgery in acute ischemic mitral regurgitation post-percutaneous coronary intervention: a case report
- PMID: 39506845
- PMCID: PMC11539844
- DOI: 10.1186/s13019-024-03019-9
Impella 5.5 as a bridge-to-surgery in acute ischemic mitral regurgitation post-percutaneous coronary intervention: a case report
Abstract
Background: Acute ischemic mitral regurgitation (AIMR) is a significant complication of acute coronary syndrome that leads to severe and immediate hemodynamic deterioration and cardiogenic shock. Intra-aortic balloon pumps (IABP) are commonly used to support patients with AIMR as a bridge to surgery, though they may be insufficient in some cases.
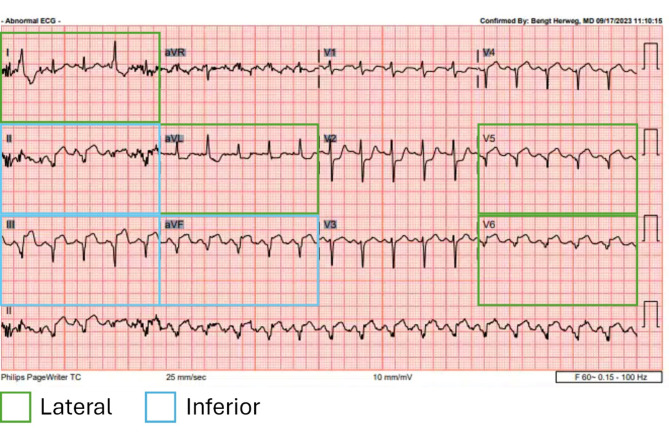
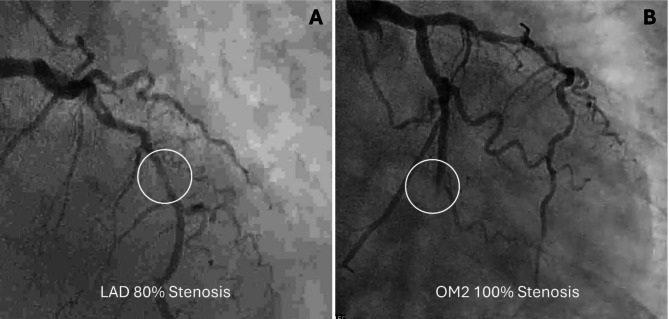
Case presentation: A 74-year-old male presented with two days of indigestion and evident hypoxia, and an electrocardiogram revealed inferior and lateral ST-elevation myocardial infarction. Angiography demonstrated severe two-vessel coronary disease with a 100% thrombotic occlusion of the second obtuse marginal artery (OM2, culprit lesion) and an 80% stenosis of the proximal left anterior descending artery (LAD). Despite stenting of OM2, the patient remained hypoxic and hypotensive, necessitating escalated support via an IABP. A follow-up echocardiogram revealed severe mitral regurgitation presumed to be AIMR secondary to a ruptured posteromedial papillary muscle with a flail anterior leaflet (A2). Despite aggressive supportive measures with the IABP, the patient's hemodynamics continued to show cardiogenic shock and clinical status did not improve. However, the patient was required to abstain from surgery for a P2Y12 inhibitor therapy wash out period. Consequently, the IABP was upgraded to Impella 5.5 as bridge-to-surgery support on day 1 post-admission. Subsequently, the patient's hemodynamics improved, and he underwent a combined mitral valve replacement and coronary artery bypass grafting surgery on day 7 post-admission without incident. The Impella was successfully explanted on day 25 post-admission. Delay in explant was due to hypotension and respiratory status despite normalizing hemodynamics and echocardiogram revealing recovered left ventricular ejection fraction. The patient developed bacterial pneumonia and acute respiratory distress syndrome and expired on day 27 post-admission.
Conclusion: Although IABP is standard for supporting AIMR patients as a bridge to surgery, it may not provide sufficient hemodynamic support. This case supports a growing body of evidence that alternative forms of hemodynamic support should be considered if the traditional therapeutic modalities for AIMR do not adequately support patients. Clinicians may consider upgrading IABP to Impella to provide increased hemodynamic support and maintain AIMR patient stability while awaiting cardiac surgery.
Keywords: Acute coronary syndrome; Cardiogenic shock; Impella; Mitral regurgitation; Temporary mechanical circulatory support.
© 2024. The Author(s).
Conflict of interest statement
Dr. Dumitru is a consultant for Abiomed. All other authors declare no conflicts of interest or disclosures concerning the generation of this manuscript.
Figures

References
-
- Vandenbriele C, Balthazar T, Wilson J, Adriaenssens T, Davies S, Droogne W, et al. Left Impella®-device as bridge from cardiogenic shock with acute, severe mitral regurgitation to MitraClip®-procedure: a new option for critically ill patients. Eur Heart J Acute Cardiovasc Care. 2021;10(4):415–21. - DOI - PubMed
-
- Bhardwaj A, Kumar S, de Armas IAS, Nascimbene A, Nathan S, Kar B et al. Pre- and post-operative mechanical circulatory support in surgical repair of post-acute myocardial infarction mechanical complications. Ann Cardiothorac Surg [Internet]. 2022 [cited 2024 Mar 13];11(3):304–9. https://pubmed.ncbi.nlm.nih.gov/35733711/ - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
