

Effective Pain Management of Postherpetic Neuralgia Using a Combination of Analgesics and Conservative Measures
- PMID: 39507605
- PMCID: PMC11539919
- DOI: 10.7759/cureus.73132
Effective Pain Management of Postherpetic Neuralgia Using a Combination of Analgesics and Conservative Measures
Abstract
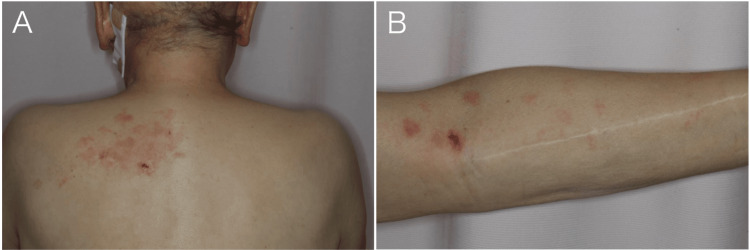
Postherpetic neuralgia (PHN) is characterized by persistent pain following the resolution of a herpes zoster rash. PHN is often resistant to treatment and can significantly reduce the patient's quality of life. Effective symptom relief is crucial and various treatments, including pharmacotherapy, have been attempted. Given that symptoms can persist for a prolonged period, they can substantially affect the physical and mental well-being of the patients. A 73-year-old man developed herpes zoster while undergoing treatment for a head angiosarcoma. Despite the resolution of the rash, the pain persisted, leading to the diagnosis of PHN. Treatment was initiated with a range of medications, including mecobalamin, pregabalin, and a combination of tramadol and acetaminophen, along with general pain relievers standardized as WHO Step 1 medications, which include acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs). However, achieving adequate pain control is challenging and results in frequent hospitalizations. Due to the patient's depression and the concurrent use of a selective serotonin reuptake inhibitor, duloxetine hydrochloride could not be prescribed. Instead, opioid therapy with continuous fentanyl citrate infusion was initiated. Eventually, the treatment was switched to oxycodone hydrochloride, which successfully stabilized the patient's symptoms. The use of conservative measures such as hot compresses also contributes to symptom relief. Alleviating pain symptoms using a combination of pharmacotherapeutic and non-pharmacological treatments is extremely important.
Keywords: duloxetine hydrochloride; hot compress; opioids; oxycodone hydrochloride; postherpetic neuralgia; pregabalin.
Copyright © 2024, Tsubaki et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- Herpes zoster and postherpetic neuralgia: prevention and management. Saguil A, Kane S, Mercado M, Lauters R. https://www.aafp.org/pubs/afp/issues/2017/1115/p656.html. Am Fam Physician. 2017;96:656–663. - PubMed
-
- Clinical practice. Postherpetic neuralgia. Johnson RW, Rice AS. N Engl J Med. 2014;371:1526–1533. - PubMed
-
- An update on the treatment of postherpetic neuralgia. Wu CL, Raja SN. J Pain. 2008;9:19–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources