

Is low-intensity shockwave therapy for erectile dysfunction a durable treatment option?-long-term outcomes of a randomized sham-controlled trial
- PMID: 39507860
- PMCID: PMC11535733
- DOI: 10.21037/tau-24-329
Is low-intensity shockwave therapy for erectile dysfunction a durable treatment option?-long-term outcomes of a randomized sham-controlled trial
Abstract
Background: Low-intensity shockwave therapy (LiSWT) is an emerging non-invasive and restorative therapy for erectile dysfunction (ED) with demonstrated efficacy and few adverse events. Although LiSWT has been shown to improve erectile function amongst men with ED, few studies have examined its long-term durability. We present the long-term results of a randomized controlled trial (RCT) assessing erectile function after LiSWT.
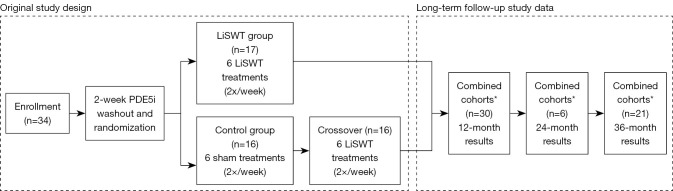
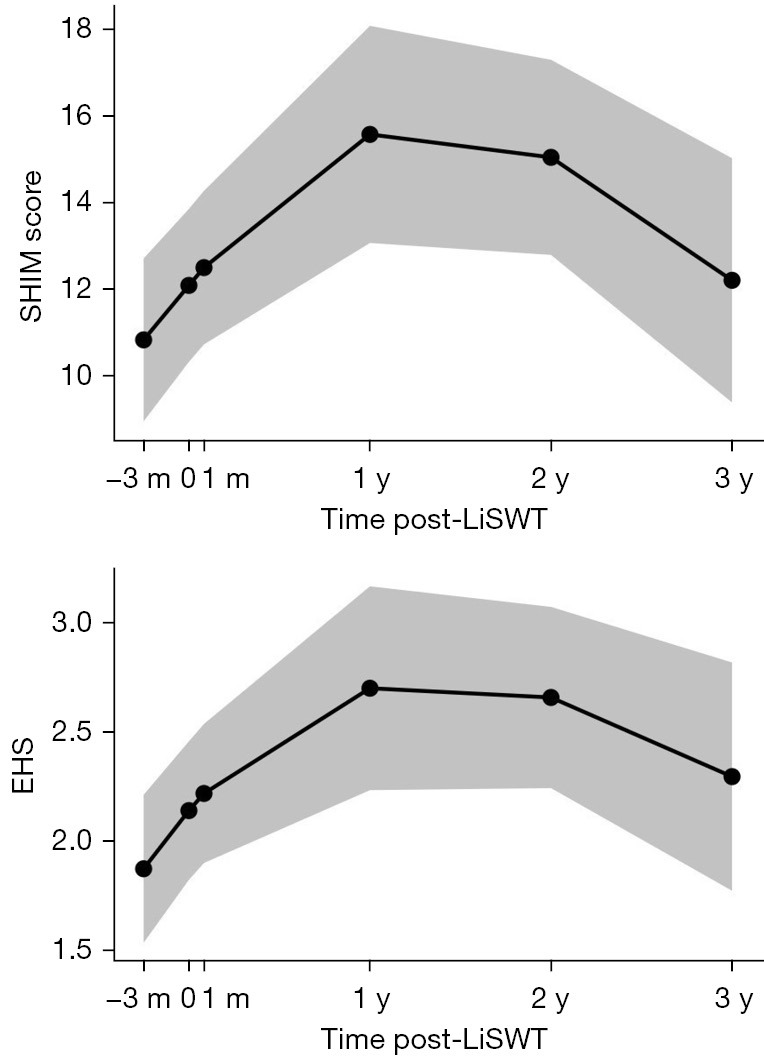
Methods: A total of 30 patients with baseline ED seen at the University of Virginia were randomized to LiSWT or sham treatment. Patients in the sham group crossed over at 1 month and were unblinded. After initial trial completion, patients enrolled in the long-term outcome study were considered one combined cohort. Patients were treated twice weekly for 3 consecutive weeks with a Storz® Duolith™ device delivering 3,000 shockwaves at 0.1 mJ/mm2 to the distal penis, the base of the penis, and the crura. Primary outcomes were changes in Sexual Health Inventory for Men (SHIM) and Erection Hardness Score (EHS) from baseline (3 months pre-treatment) up to 36 months post-treatment. Changes in SHIM and EHS scores were evaluated using linear mixed effects models. Patient satisfaction was assessed with the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS) index.
Results: The mean baseline SHIM score was 10.8±0.94. At 12-, 24-, and 36-month assessment following treatment, the mean SHIM scores were 15.6±1.27 (P<0.001), 15.0±1.14 (P<0.001), and 12.2±1.43 (P=0.31). The mean baseline EHS score was 1.87±0.17. At 12-, 24-, and 36-month assessment following treatment, the mean EHSs were 2.70±0.24 (P<0.001), 2.66±0.21 (P<0.001), and 2.29±0.26 (P=0.10). The median [interquartile range (IQR)] EDITS score was 48.9 (22.7, 74.4), indicating moderate satisfaction with LiSWT. There were no adverse events recorded.
Conclusions: Our analysis demonstrates sustained long-term improvement in erectile function after LiSWT for a heterogeneous cohort. While limited by population size, the results suggest durable improvement in erectile function for the first 2 years with a peak treatment effect at 1 year. Treatment effect appears to decline between 2 and 3 years.
Clinical trial registration: ClinicalTrials.gov, NCT04434352.
Keywords: Sexual dysfunction, physiological; erectile dysfunction (ED); extracorporeal shockwave therapy; psychological; sexual dysfunction; urogenital diseases.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tau.amegroups.com/article/view/10.21037/tau-24-329/coif). R.S. serves as an unpaid editorial board member of the Translational Andrology and Urology from August 2024 to July 2026, and serves as the Chief Medical Officer of PS Fertility, LLC. The other authors have no conflicts of interest to declare.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical