

Hereditary Angioedema Attacks in Patients Receiving Long-Term Prophylaxis: A Systematic Review
- PMID: 39508959
- PMCID: PMC11638394
- DOI: 10.1007/s12016-024-09006-1
Hereditary Angioedema Attacks in Patients Receiving Long-Term Prophylaxis: A Systematic Review
Abstract
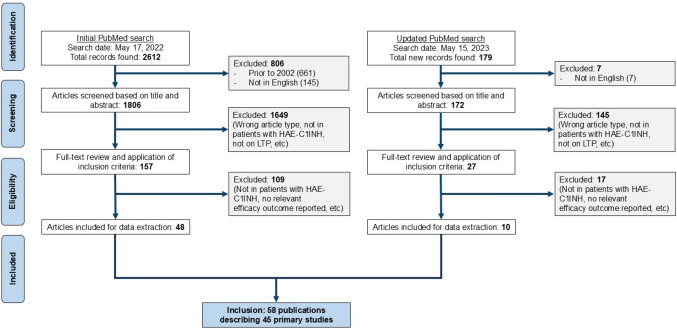
Long-term prophylaxis (LTP) has been shown to reduce the frequency of hereditary angioedema (HAE) attacks; however, attacks occurring in patients receiving LTP have not been well characterized. The objective of this systematic review was to evaluate the proportion of type I/II HAE (HAE-C1INH) patients who experience attacks while receiving LTP, the characteristics of these attacks, and associated on-demand therapy use. A systematic search was conducted in PubMed to identify studies reporting LTP use with plasma-derived C1 inhibitor (pdC1INH), lanadelumab, berotralstat, androgens, or antifibrinolytics in patients with HAE-C1INH. Forty-five primary studies met the inclusion criteria. In phase 3 trials, attack-free rates were 40% for subcutaneous pdC1INH 60 IU/kg twice weekly at 16 weeks, and 44% for lanadelumab 300 mg every second week at 6 months (77% during steady-state [days 70-182]); there was no difference in attack-free rate for berotralstat 150 mg versus placebo at 24 weeks. Phase 3 studies reported a lower average attack severity with subcutaneous and intravenous pdC1INH versus placebo. With lanadelumab and berotralstat, the prophylactic treatment effect was more pronounced in peripheral attacks than in abdominal and laryngeal attacks. Laryngeal attacks accounted for 2%-7% of all attacks in observational and interventional studies, regardless of the LTP agent received. On-demand therapy was used in 49%-94% of attacks occurring in the presence of LTP. In conclusion, patients receiving LTP experienced attacks in all anatomic locations, including the larynx. Most attacks were treated with on-demand therapy, although outcomes were not reported. Access to on-demand therapy remains essential for all people with HAE-C1INH.
Keywords: Attack-free rate; Hereditary angioedema; Long-term prophylaxis; On-demand therapy; Systematic review.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics Approval: Not applicable for this literature review. Competing Interests: H. J. Longhurst has received grants or contracts from CSL Behring, Intellia, and KalVista, consulting fees from CSL Behring, Intellia, KalVista, and Takeda, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from CSL Behring and Takeda, support for travel and/or attending meetings from CSL Behring, Intellia, KalVista, Pharming, and Takeda, has participated on a Data Safety Monitoring Board or Advisory Board for CSL Behring, Intellia, KalVista, and Takeda, has received equipment, materials, drugs, medical writing, gifts or other services from CSL Behring, Intellia, KalVista, and has held a leadership or fiduciary role in HAE International Scientific Steering Committees. L. Bouillet has received support for the medical writing of this manuscript which was funded by KalVista, has received consulting fees from Takeda, CSL Behring, BioCryst, and KalVista, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from Takeda and BioCryst, payment for expert testimony from Takeda, CSL Behring, Pharvaris, BioCryst, and KalVista, support for travel and/or attending meetings from Takeda and BioCryst, has participated on a Data Safety Monitoring Board or Advisory Board for Takeda, BioCryst, CSL Behring, KalVista, and Pharvaris, and is the vice-president of the Société Nationale Française de Médecine Interne (SNFMI). M. Cancian has received consulting fees from CSL Behring, Takeda, Pharvaris, KalVista, and BioCryst, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from KalVista, Takeda, and CSL Behring, and support for travel and/or attending meetings from CSL Behring and Takeda. V. Grivcheva-Panovska has received support for the medical writing of this manuscript which was funded by KalVista, consulting fees from Pharming NV, KalVista, Astria, and Takeda, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from Pharming NV, Takeda, BioCryst, and KalVista, travel grants from Pharming NV and Takeda, has participated on a Data Safety Monitoring Board or Advisory Board for Pharming NV, KalVista, Takeda, and Astria and has received medical writing assistance from Pharming NV, BioCryst, and KalVista. M Koleilat has received support for the medical writing of this manuscript which was funded by KalVista, and has received grants or contracts as a clinical trial site from KalVista. M. Magerl has received support for medical writing of this manuscript which was funded by KalVista, research funding as a study center investigator from KalVista, and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from CSL Behring, Shire/Takeda, Pharming Technologies, BioCryst, Novartis, Octapharma, KalVista, Intellia, and Pharvaris. S. Savic has received support for the present manuscript from KalVista, grants or contracts from Novartis, SOBI, and CSL Behring, consulting fees from Novartis, SOBI, CSL Behring, Takeda, KalVista, BioCryst, Pharming, Celdex, and AstraZeneca, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from Takeda, SOBI, Novartis, and KalVista, has received support for travel and/or attending meetings from Novartis, and has a leadership or fiduciary role for the British Society for Immunology. M. Stobiecki has received lecture and presentations honoraria and consulting fees from CSL Behring, Takeda/Shire, and BioCryst. R Tachdjian has received grants or contracts from Astria, Ionis, CSL Behring, BioCryst, Takeda, KalVista, and Pharvaris, consulting fees from BioCryst, CSL Behring, Pharming, Takeda, KalVista, and Ionis, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from BioCryst, CSL Behring, Pharming, Takeda, Ionis, Sanofi, Regeneron, AstraZeneca, and GlaxoSmithKline, and has participated on a Data Safety Monitoring Board or Advisory Board for Astria, BioCryst, CSL Behring, KalVista, Pharming, Takeda, and Ionis. B. Healy is an employee of ApotheCom, which received funding from KalVista Pharmaceuticals for the project and support for travel and/or meeting attendance from KalVista Pharmaceuticals. C. M. Yea and P. K. Audhya hold stock or stock options and are employees of KalVista Pharmaceuticals.
Figures
References
-
- Busse PJ, Christiansen SC, Riedl MA, Banerji A, Bernstein JA, Castaldo AJ, Craig T, Davis-Lorton M, Frank MM, Henry Li H, Lumry WR, Zuraw BL (2021) US HAEA Medical Advisory Board 2020 guidelines for the management of hereditary angioedema. J Allergy Clin Immunol Pract 9:132–50.e3. 10.1016/j.jaip.2020.08.046 - DOI - PubMed
-
- Bork K, Anderson JT, Caballero T, Craig T, Johnston DT, Li HH, Longhurst HJ, Radojici C, Riedl M (2021) Assessment and management of disease burden and quality of life in patients with hereditary angioedema: a consensus report. Allergy Asthma Clin Immunol 17:40. 10.1186/s13223-021-00537-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
