

Convergent and divergent immune aberrations in COVID-19, post-COVID-19-interstitial lung disease, and idiopathic pulmonary fibrosis
- PMID: 39510135
- PMCID: PMC12204034
- DOI: 10.1152/ajpcell.00528.2024
Convergent and divergent immune aberrations in COVID-19, post-COVID-19-interstitial lung disease, and idiopathic pulmonary fibrosis
Abstract
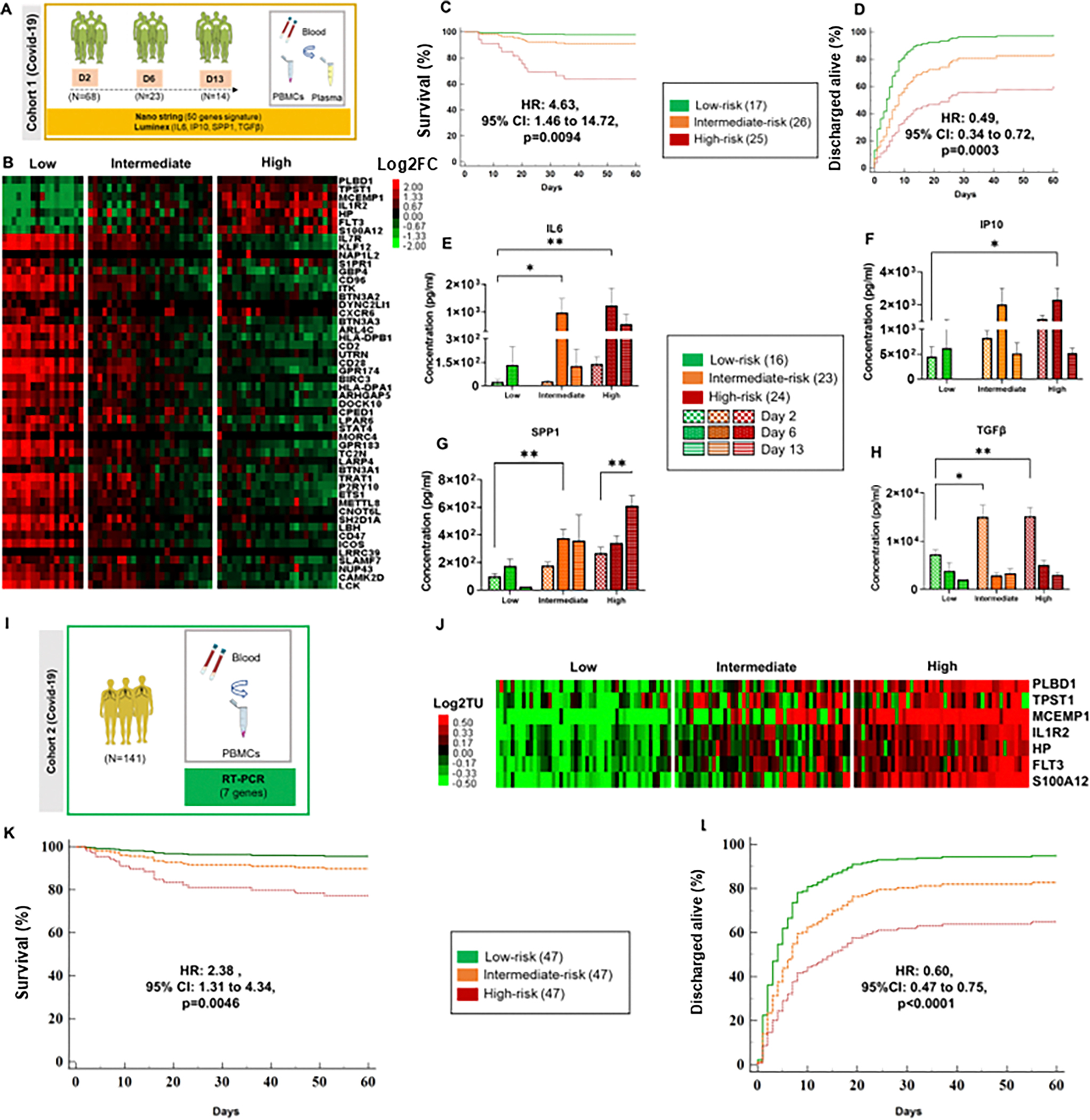
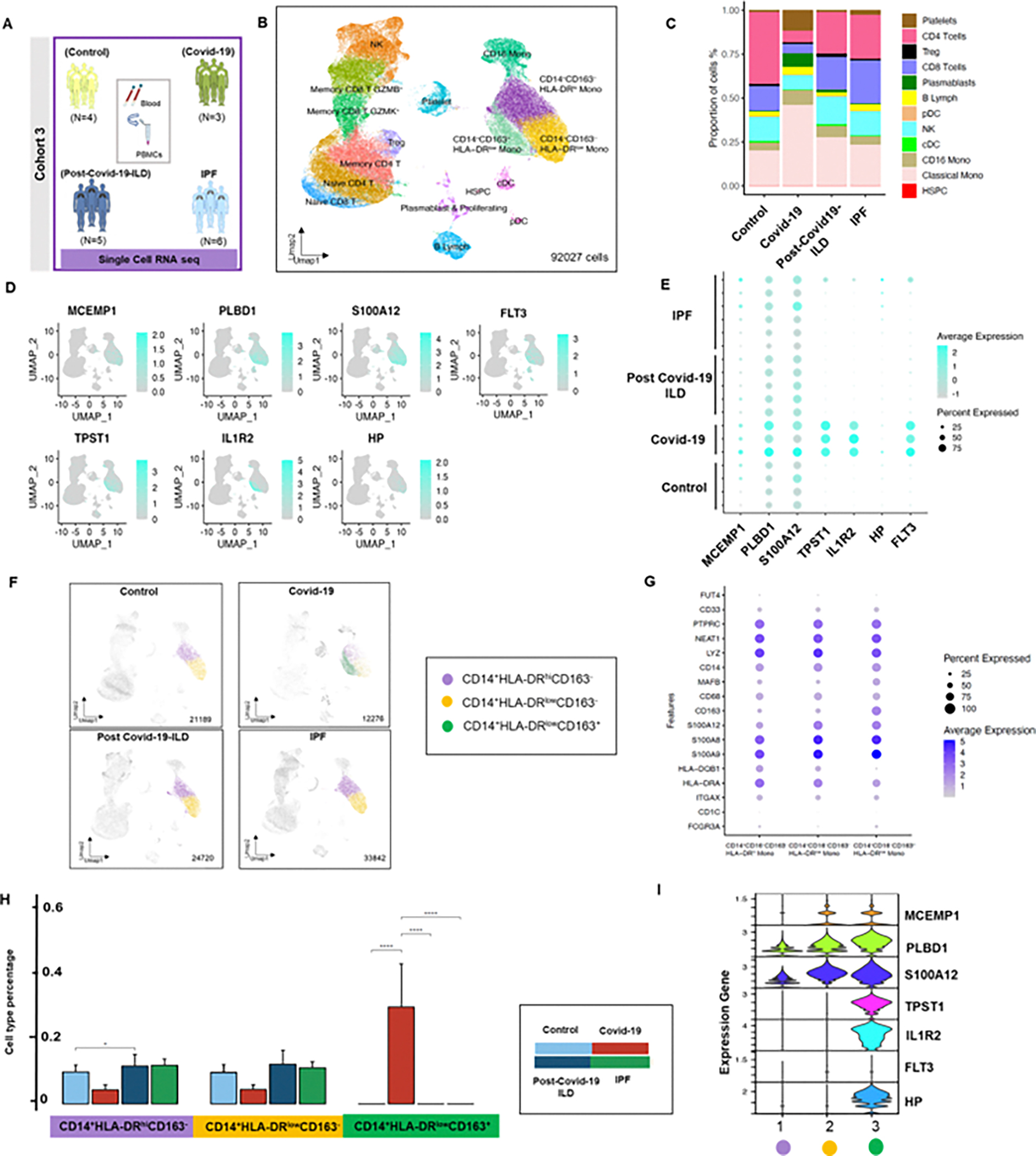
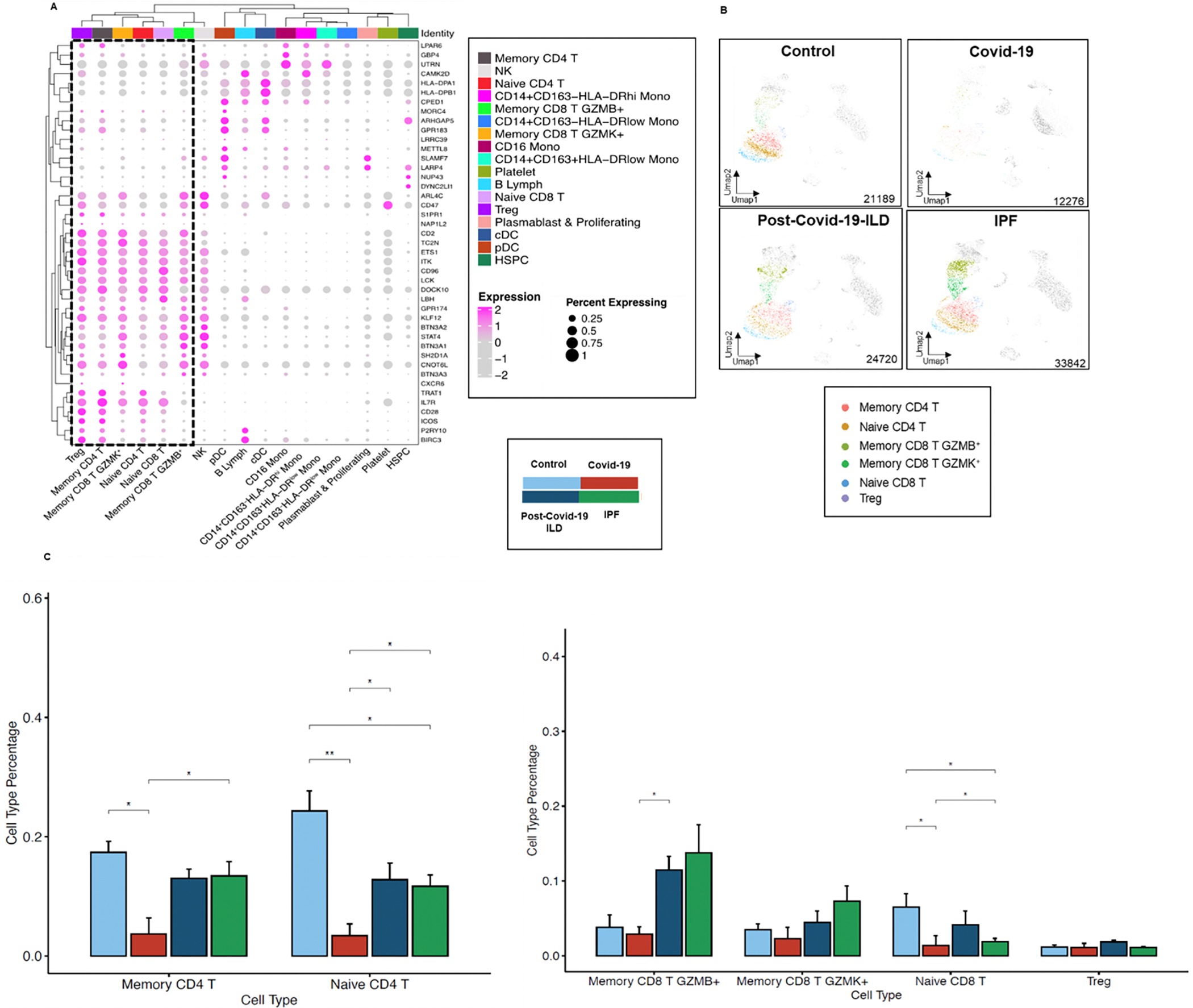
We aimed to study transcriptional and phenotypic changes in circulating immune cells associated with increased risk of mortality in COVID-19, resolution of pulmonary fibrosis in post-COVID-19-interstitial lung disease (ILD), and persistence of idiopathic pulmonary fibrosis (IPF). Whole blood and peripheral blood mononuclear cells (PBMCs) were obtained from 227 subjects with COVID-19, post-COVID-19 interstitial lung disease (ILD), IPF, and controls. We measured a 50-gene signature (nCounter, Nanostring) previously found to be predictive of IPF and COVID-19 mortality along with plasma levels of several biomarkers by Luminex. In addition, we performed single-cell RNA sequencing (scRNA-seq) in PBMCs (10x Genomics) to determine the cellular source of the 50-gene signature. We identified the presence of three genomic risk profiles in COVID-19 based on the 50-gene signature associated with low-, intermediate-, or high-risk of mortality and with significant differences in proinflammatory and profibrotic cytokines. Patients with COVID-19 in the high-risk group had increased expression of seven genes in CD14+HLA-DRlowCD163+ monocytic-myeloid-derived suppressive cells (7Gene-M-MDSCs) and decreased expression of 43 genes in CD4 and CD8 T cell subsets. The loss of 7Gene-M-MDSCs and increased expression of these 43 genes in T cells was seen in survivors with post-COVID-19-ILD. On the contrary, patients with IPF had low expression of the 43 genes in CD4 and CD8 T cells. Collectively, we showed that a 50-gene, high-risk profile, predictive of IPF and COVID-19 mortality is characterized by a genomic imbalance in monocyte and T-cell subsets. This imbalance reverses in survivors with post-COVID-19-ILD highlighting genomic differences between post-COVID-19-ILD and IPF.NEW & NOTEWORTHY Changes in the 50-gene signature, reflective of increase in CD14+HLA-DRlowCD163+ monocytes and decrease in CD4 and CD8 T cells, are associated with increased mortality in COVID-19. A reversal of this pattern can be seen in post-COVID-19-ILD, whereas its persistence can be seen in IPF. Modulating the imbalance between HLA-DRlow monocytes and T cell subsets should be investigated as a potential strategy to treat pulmonary fibrosis associated with severe COVID-19 and progressive IPF.
Keywords: 50-gene signature; 7Gene-M-MDSCs; COVID-19; IPF; post-COVID-19-ILD.
Conflict of interest statement
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials