

Structures, processes and outcomes between first referral and referral hospitals in low-income and middle-income countries: a secondary preplanned analysis of the FALCON and ChEETAh randomised trials
- PMID: 39510564
- PMCID: PMC11552540
- DOI: 10.1136/bmjgh-2024-015599
Structures, processes and outcomes between first referral and referral hospitals in low-income and middle-income countries: a secondary preplanned analysis of the FALCON and ChEETAh randomised trials
Abstract
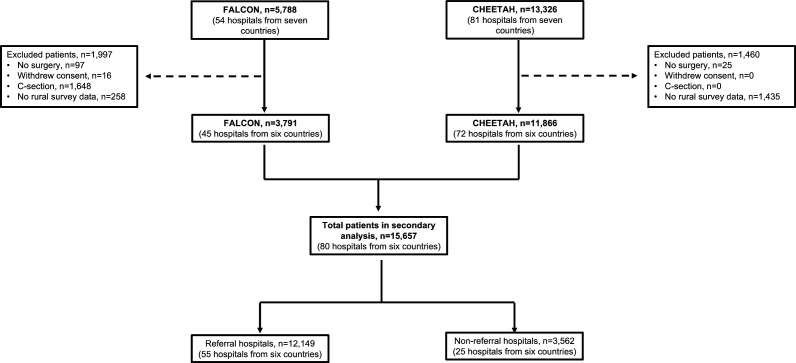
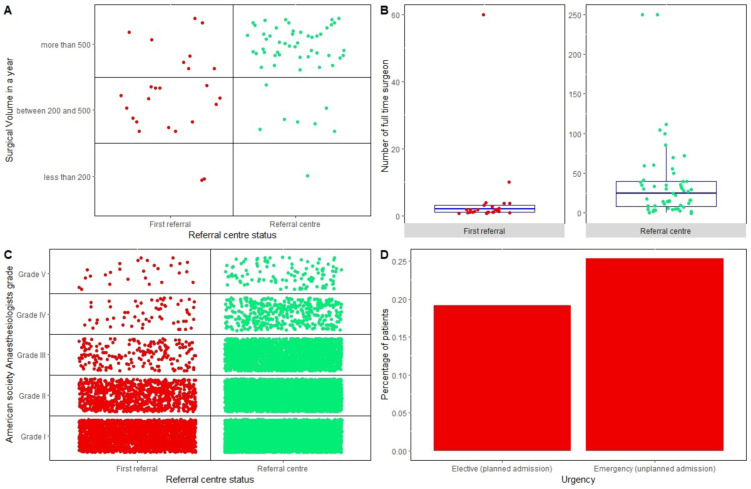
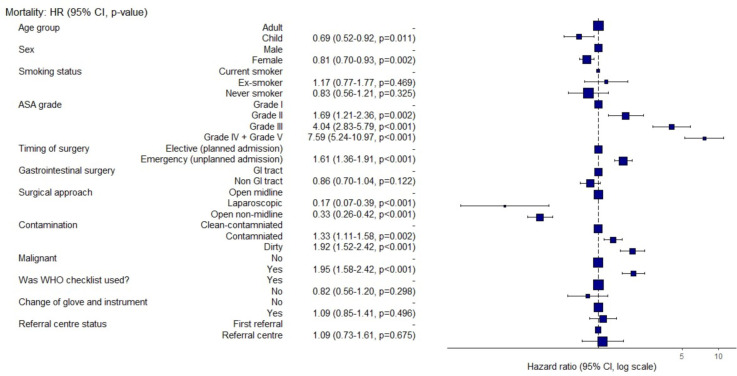
First referral hospitals, often known as district hospitals, are neglected in the discourse on universal health coverage in low-income and middle-income countries (LMICs). However, these hospitals are important for delivering safe surgery for 313 million people. This study aims to understand the structures, processes and outcomes of patients undergoing surgery in these centres in LMICs. This is a preplanned secondary analysis using data from two high-quality randomised controlled trials undergoing major abdominal surgery across six LMICs. Type of hospital was the main explanatory variable, defined according to the WHO taxonomy as first referral (ie, district or rural) and referral (ie, secondary or tertiary). Of the included 15 657 patients across 80 hospitals from 6 countries, 3562 patients underwent surgery in first referral and 12 149 patients underwent surgery in referral centres. First referral centres have lower full-time surgeons (median: 1 vs 20, p<0.001) and medically trained anaesthetists (28.6% vs 87.1%, p<0.001) compared with referral centres. Patients undergoing surgery in first referral centres were more likely to have lower rates of American Society of Anaesthesiologist (ASA) grades III-V (8.1% vs 22.7%, p<0.001), but higher rates of emergency procedures (65.1% vs 56.6%, p<0.001). In first referral centres, there was a significantly higher use of WHO surgical safety checklist (99.4% vs 93.3%, p<0.001) compared with referral centres. In adjusted analyses, there were no differences in 30-day mortality (OR 1.09, 95% CI 0.73 to 1.62) and surgical site infection (OR 1.30, 95% CI 0.89 to 1.90) between first referral and referral centres. Postoperative mortality and surgical site infection remain similar between first referral and referral centres in LMICs. There may be a clear need to upscale surgical volume safely in first referral centres to meet global surgical needs. High-quality research is needed to drive safe expansion of surgical workforce and strengthen referral pathways within these surgical health systems in LMICs.
Keywords: Surgery.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources