

Postoperative tumor bed radiation versus T-shaped field radiation in the treatment of locally advanced thoracic esophageal squamous cell carcinoma: a phase IIb multicenter randomized controlled trial
- PMID: 39511550
- PMCID: PMC11545895
- DOI: 10.1186/s12916-024-03727-y
Postoperative tumor bed radiation versus T-shaped field radiation in the treatment of locally advanced thoracic esophageal squamous cell carcinoma: a phase IIb multicenter randomized controlled trial
Abstract
Background: Postoperative radiotherapy (PORT) is crucial for patients with thoracic locally advanced esophageal squamous cell carcinoma (LA-ESCC, pT3-4aN0-3M0) following esophagectomy. However, the appropriate radiation volume has not been well established. This study aimed to determine the optimal PORT volume for LA-ESCC patients.
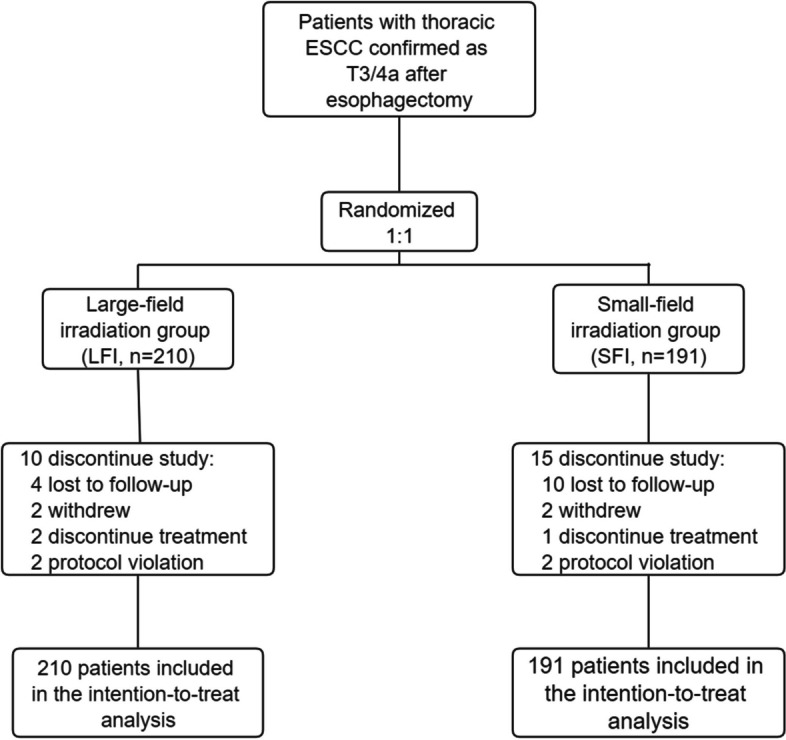
Methods: LA-ESCC patients post-esophagectomy were randomly assigned to either the large-field irradiation (LFI, primary lesion and lymph node tumor bed plus elective nodal irradiation) group or the small-field irradiation (SFI, primary lesion and lymph node tumor bed alone) group. Stratification was based on T stage and the number of lymph node metastases. The primary endpoint was disease-free survival (DFS), while the secondary endpoints included overall survival (OS), adverse events, and patterns of initial failure.
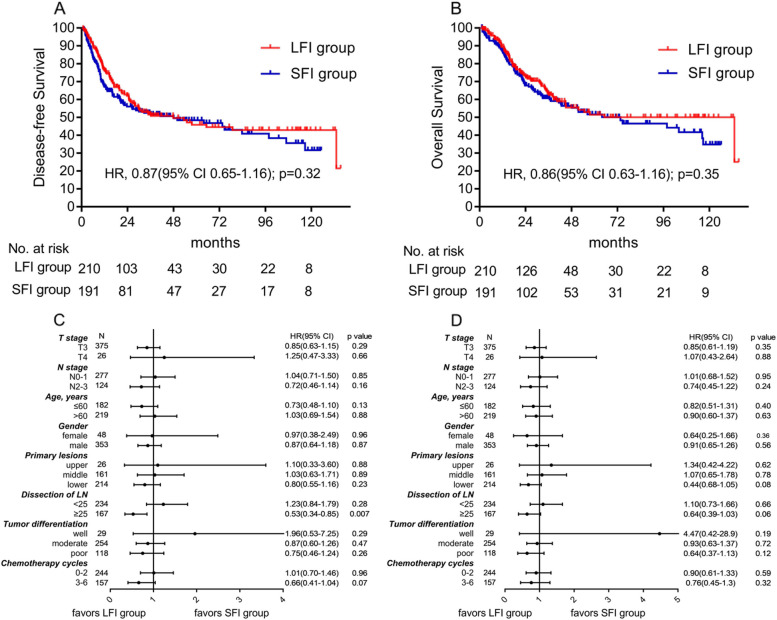
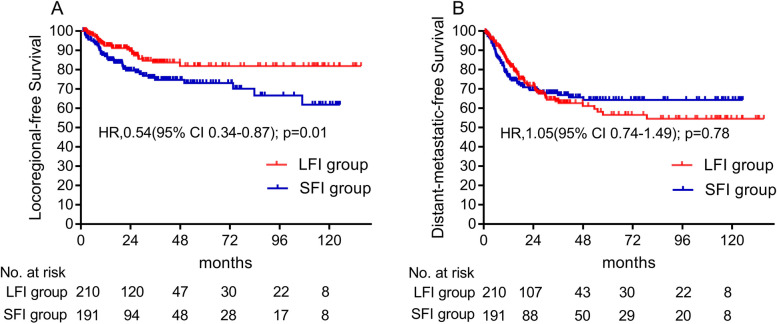
Results: A total of 401 patients were randomly assigned to the intention-to-treat analysis(LFI group, n = 210; SFI group, n = 191). The median DFS of patients in the LFI group was 47.9 months and 48.1 months in the SFI group (HR = 0.87, 95%CI, 0.65 to 1.16; p = 0.32). The estimated one-year and three-year OS rates were 89.2% and 63.2% for patients in the LFI group, compared to 86.6% and 60.7% for the SFI group, respectively. The difference of OS between the two groups was not significant (HR = 0.86, 95%CI, 0.63 to 1.16; p = 0.35). Fewer patients in the LFI group experienced locoregional recurrence compared to the SFI group (12.9% vs 20.4%, p = 0.013). Additionally, locoregional recurrence-free survival of the LFI group was significantly longer than that of SFI group (HR = 0.54, 95%CI, 0.34-0.87; p = 0.01). The most common toxicity was grade 2 esophagitis, observed in 22.9% of the LFI group and 16.8% of the SFI group. Grade 3 adverse events occurred in 6.7% of the LFI group and 2.6% of the SFI group. No grade 4 or 5 toxicities were observed. Adverse events did not significantly differ between the two groups.
Conclusions: Postoperative radiotherapy, with the specified radiation volume shows encouraging survival outcomes that are comparable to those of neoadjuvant chemoradiotherapy in patients with thoracic LA-ESCC. Both postoperative irradiation fields were found to be feasible and safe.
Keywords: Locally advanced esophageal squamous cell carcinoma; Locoregional control; Postoperative radiotherapy; Radiation volume; Survival outcomes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–84. - PubMed
-
- Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16:1090–8. - PubMed
-
- Mao YS, Gao SG, Wang Q, Shi XT, Li Y, Gao WW, et al. Epidemiological characteristic and current status of surgical treatment for esophageal cancer by analysis of national registry database. Zhonghua zhong liu za zhi (Chinese Journal of Oncology). 2020;42:228–33. - PubMed
-
- Zhang W, Liu X, Xiao Z, Zhang H, Chen D, Feng Q, et al. Postoperative intensity-modulated radiotherapy improved survival in lymph node-positive or stage III thoracic esophageal squamous cell carcinoma. Oncol Res Treat. 2015;38:97–102. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
