

High-risk plaques in non-culprit lesions and clinical outcome after NSTEMI vs. STEMI
- PMID: 39512201
- PMCID: PMC11781827
- DOI: 10.1093/ehjci/jeae289
High-risk plaques in non-culprit lesions and clinical outcome after NSTEMI vs. STEMI
Abstract
Aims: Complete non-culprit (NC) revascularisation may help reduce recurrent events after non-ST-segment elevation myocardial infarction (NSTEMI), especially if NC lesions would harbour high-risk plaque (HRP) features similar to ST-segment elevation myocardial infarction (STEMI). This study aimed to assess differences in fractional flow reserve (FFR)-negative NC plaque morphology in patients presenting with NSTEMI vs. STEMI and assess the association of HRP morphology and clinical outcome.
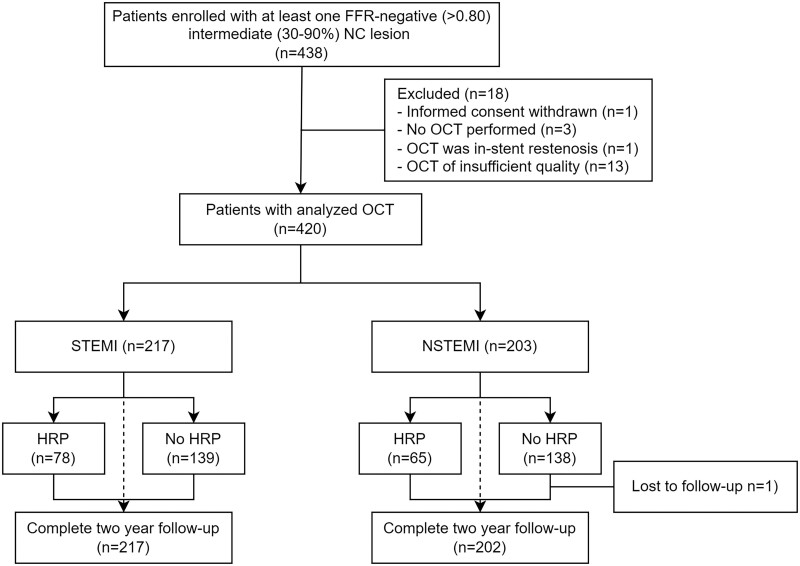
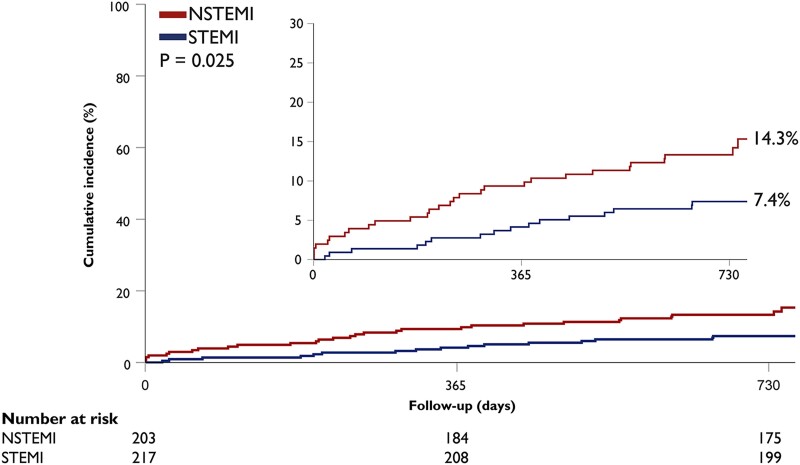
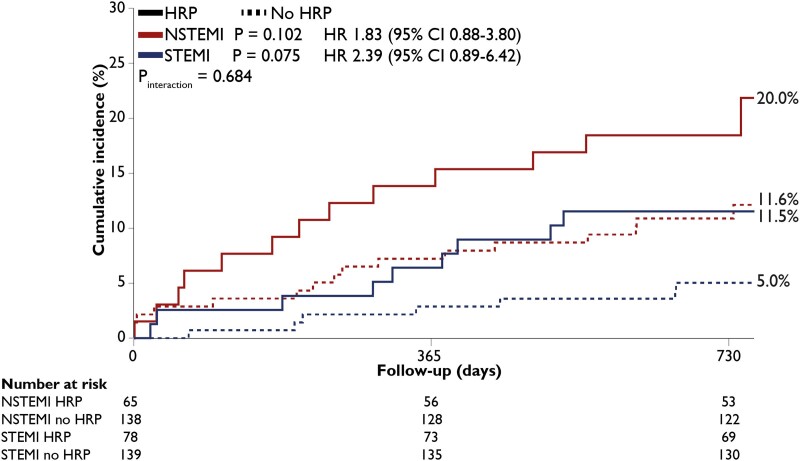
Methods and results: In the prospective PECTUS-obs study, 438 patients presenting with myocardial infarction (MI) underwent optical coherence tomography (OCT) of all FFR-negative intermediate NC lesions. The primary endpoint was the occurrence of major adverse cardiovascular events (MACE, composite of all-cause mortality, non-fatal MI or unplanned revascularisation) at 2-year follow-up. Four hundred and twenty patients had at least one analysable OCT, including 203 (48.3%) with NSTEMI and 217 (51.7%) with STEMI. The prevalence of HRPs, including thin-cap fibroatheromas, plaque rupture, and thrombus, was comparable between groups. MACE occurred in 29 (14.3%) NSTEMI patients and 16 (7.4%) STEMI patients (Puni-variable = 0.025 and Pmulti-variable = 0.270). Incidence of MACE was numerically higher among patients with HRP, irrespective of the clinical presentation at index (Pinteraction = 0.684). Among HRP criteria, plaque rupture was associated with MACE in both NSTEMI (P < 0.001) and STEMI (P = 0.020).
Conclusion: Presence of NC HRP is comparable between NSTEMI and STEMI and leads to numerically higher event rates in both. These results call for additional research on complete revascularisation in NSTEMI and treatment of HRP.
Clinical trial registration: NCT03857971.
Keywords: NSTEMI; STEMI; TCFA; fractional flow reserve; high-risk plaque; non-culprit; plaque rupture.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: R.H.J.A.V. reported receiving grant funding from Abbott Vascular and Health~Holland during the conduct of the study. J.-Q.M. reported receiving grant funding from Abbott Vascular and Health~Holland during the conduct of the study. A.B. reported receiving speaker’s fees from Daiichi Sankyo Inc, travel fees from Novo Nordisk and Daiichi Sankyo, and is shareholder of Pfizer, outside the submitted work. R.S.H. reported receiving speaker fees from Amgen Inc, Angiocare, Edwards Lifesciences and Novartis AG outside the submitted work. R.M.O. reported receiving speaker fees from Abbott Vascular outside the submitted work. E.L. reported receiving grant funding from Abbott Laboratories outside the submitted work. C.C. reported receiving honorarium for organizing regional meetings from AstraZeneca outside the submitted work. P.D. reported receiving grant funding from Abbott Laboratories, AstraZeneca and Philips, ans consulting fees from Abbott Laboratories outside the submitted work. E.K. reported receiving grant funding from Abbott Laboratories and Medtronic, and proctorship honoraria from Abbott laboratories outside the submitted work. M.A.H.v.L. reported receiving grant funding from AstraZeneca, Top Sector Life Sciences & Health, Terumo Corporation, TOP Medical BV, and Abbott Laboratories and speakers’ fees and consulting from Terumo Corporation, Daiichi Sankyo Inc, and Abbott Laboratories outside the submitted work. R.-J.M.v.G. reported receiving grant funding from InfraRedx, and speaker fees from Amgen and Sanofi outside the submitted work. N.v.R. reported receiving grant funding and personal fees from Abbott Vascular and Health~Holland during the conduct of the study and grants from Philips, Biotronik, and Medtronic Inc, and speaker fees from Bayer AG, MicroPort, and RainMed Medical outside the submitted work.
Figures

References
-
- Chan MY, Sun JL, Newby LK, Shaw LK, Lin M, Peterson ED et al. Long-term mortality of patients undergoing cardiac catheterization for ST-elevation and non-ST-elevation myocardial infarction. Circulation 2009;119:3110–7. - PubMed
-
- Biswas S, Andrianopoulos N, Papapostolou S, Noaman S, Duffy SJ, Lefkovits J et al. Does the subtype of acute coronary syndrome treated by percutaneous coronary intervention predict long-term clinical outcomes? Eur Heart J Qual Care Clin Outcomes 2018;4:318–27. - PubMed
-
- van Leeuwen MA, Daemen J, van Mieghem NM, de Boer SP, Boersma E, van Geuns RJ et al. Comparison of long-term outcomes in STEMI and NSTE-ACS after coronary stent placement: an analysis in a real world BMS and DES population. Int J Cardiol 2013;167:2082–7. - PubMed
-
- Iannaccone M, Quadri G, Taha S, D'Ascenzo F, Montefusco A, Omede P et al. Prevalence and predictors of culprit plaque rupture at OCT in patients with coronary artery disease: a meta-analysis. Eur Heart J Cardiovasc Imaging 2016;17:1128–37. - PubMed
-
- Dong L, Mintz GS, Witzenbichler B, Metzger DC, Rinaldi MJ, Duffy PL et al. Comparison of plaque characteristics in narrowings with ST-elevation myocardial infarction (STEMI), non-STEMI/unstable angina pectoris and stable coronary artery disease (from the ADAPT-DES IVUS substudy). Am J Cardiol 2015;115:860–6. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
