

Long-Term Outcomes of Patients With Apical Hypertrophic Cardiomyopathy Utilizing a New Risk Score
- PMID: 39512540
- PMCID: PMC11540864
- DOI: 10.1016/j.jacadv.2024.101235
Long-Term Outcomes of Patients With Apical Hypertrophic Cardiomyopathy Utilizing a New Risk Score
Abstract
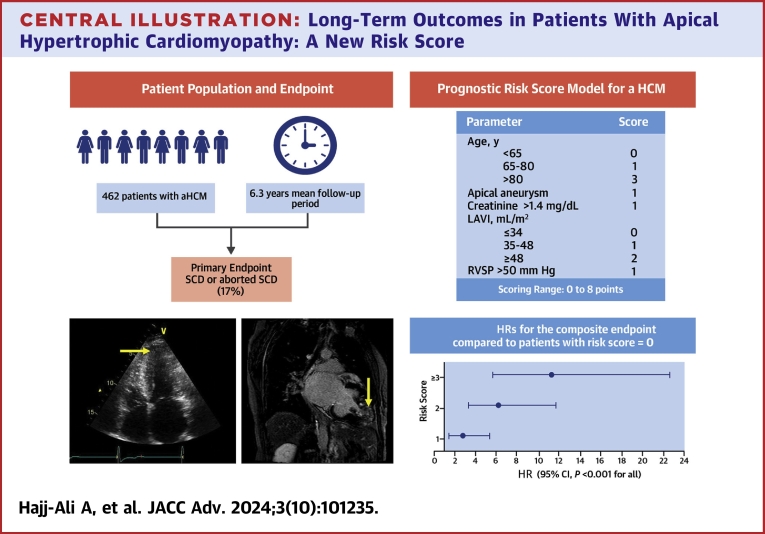
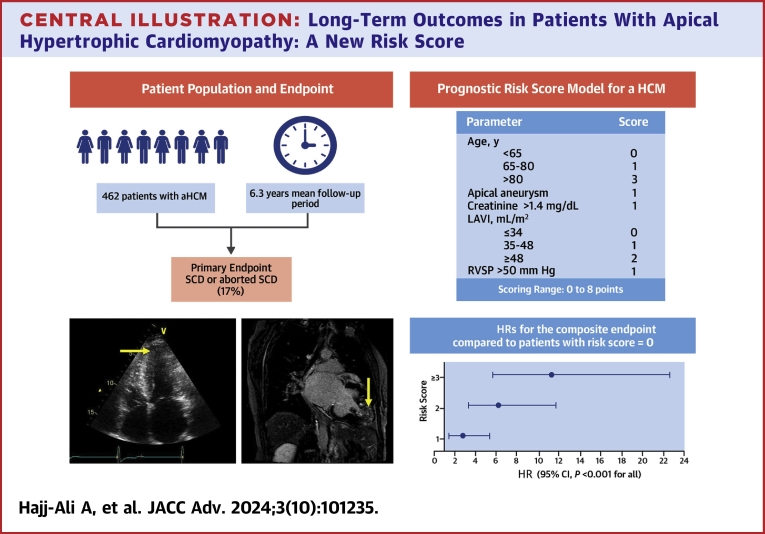
Background: Apical hypertrophic cardiomyopathy (aHCM) is a distinct variant characterized by predominant hypertrophy of the left ventricle apex.
Objectives: This study sought to describe aHCM patients' characteristics and develop a risk score for aHCM patients.
Methods: A total of 462 patients (age 58 ± 15 years, 68% male) diagnosed with aHCM were included. The primary endpoint was death, appropriate defibrillator discharge, or need for cardiac transplantation. Variables showing potential association with the composite endpoint were considered to develop an aHCM-specific risk score.
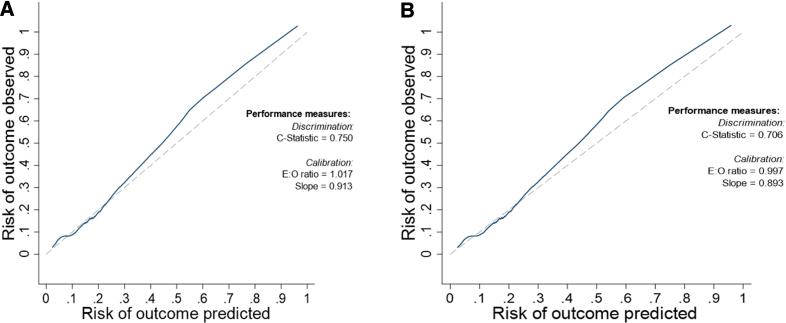
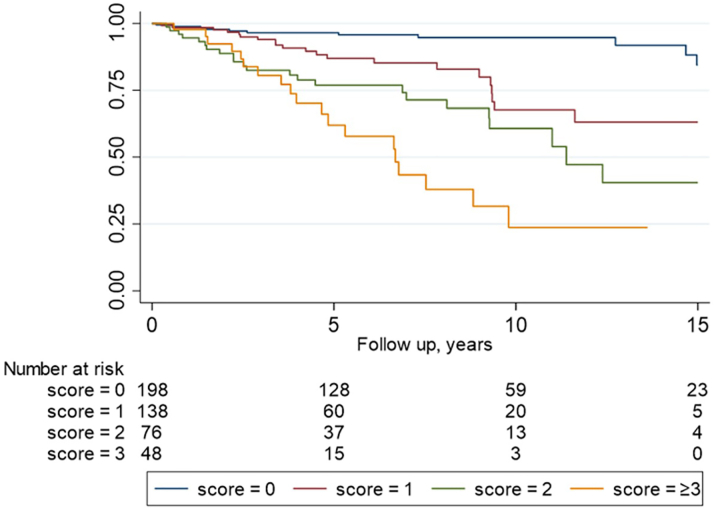
Results: At baseline, 67% patients were asymptomatic and 69% had no risk factors for sudden death. On echocardiography, the mean left ventricle ejection fraction, left atrial volume index, and right ventricular systolic pressure were 64% ± 8%, 36 ± 15 ml/m2, and 32 ± 10 mm Hg, respectively, with 51(11%) demonstrating an apical aneurysm. Baseline cardiac magnetic resonance, performed in 246 (53%) patients, demonstrated delayed gadolinium enhancement in 170 (71%) patients (mean percentage of 4.9% ± 6.6%). At age 6.3 ± 4.8 years, the composite events occurred in 80 (17%, death in 62 [13%]) patients. The aHCM-specific risk score, incorporating age, apical aneurysm, left atrial volume index, serum creatinine, and right ventricular systolic pressure, demonstrated good discrimination (C-statistic = 0.75) with an expected to observed ratio of 1.02 and a calibration slope of 0.91. The risk score ranged between 0 and 8 points, with a higher score associated with higher composite events.
Conclusions: aHCM constituted 6.8% of our overall HCM cohort with a composite event rate of 2.8%/year. The aHCM risk score provided good discrimination in predicting the composite primary endpoint, with a higher score associated with a higher rate of events.
Keywords: apical hypertrophic cardiomyopathy; prognosis; risk score.
© 2024 The Authors.
Conflict of interest statement
The current study was funded by unrestricted philanthropic gifts by the Ratner family, Stinson family, and Anderson family for Dr Desai’s research. Dr Hajj-Ali, Dr Gaballa, Mrs Ospina, and Dr Jadam have received salary support from unrestricted philanthropic gifts by the Haslam family, Ratner family, Stinson family, and Anderson family. Dr Desai is a consultant and has research agreements with Bristol Myers Squibb, Cytokinetics, Tenaya, Viz-AI, and Edgewise. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Arbelo E., Protonotarios A., Gimeno J.R., et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44:3503–3626. - PubMed
-
- Ommen S.R., Mital S., Burke M.A., et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2020;76:e159–e240. - PubMed
-
- Maron B.J., Desai M.Y., Nishimura R.A., et al. Diagnosis and evaluation of hypertrophic cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2022;79:372–389. - PubMed
-
- Sakamoto T., Tei C., Murayama M., et al. Giant T wave inversion as a manifestation of asymmetrical apical hypertrophy (AAH) of the left ventricle echocardiographic and ultrasono-cardiotomographic study. Jpn Heart J. 1976;17:611–629. - PubMed
-
- Klarich K.W., Attenhofer Jost C.H., Binder J., et al. Risk of death in long-term follow-up of patients with apical hypertrophic cardiomyopathy. Am J Cardiol. 2013;111:1784–1791. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
