

Impact of Residual Transmitral Mean Pressure Gradient on Outcomes After Mitral Transcatheter Edge-to-Edge Repair
- PMID: 39512541
- PMCID: PMC11540861
- DOI: 10.1016/j.jacadv.2024.101227
Impact of Residual Transmitral Mean Pressure Gradient on Outcomes After Mitral Transcatheter Edge-to-Edge Repair
Abstract
Background: There is conflicting evidence regarding the effect of residual transmitral mean pressure gradient (TMPG) after mitral transcatheter edge-to-edge repair (M-TEER). Different TMPG cutoffs have been employed in prior studies with varying results.
Objectives: The purpose of this study was to examine the association between residual TMPG and M-TEER outcomes.
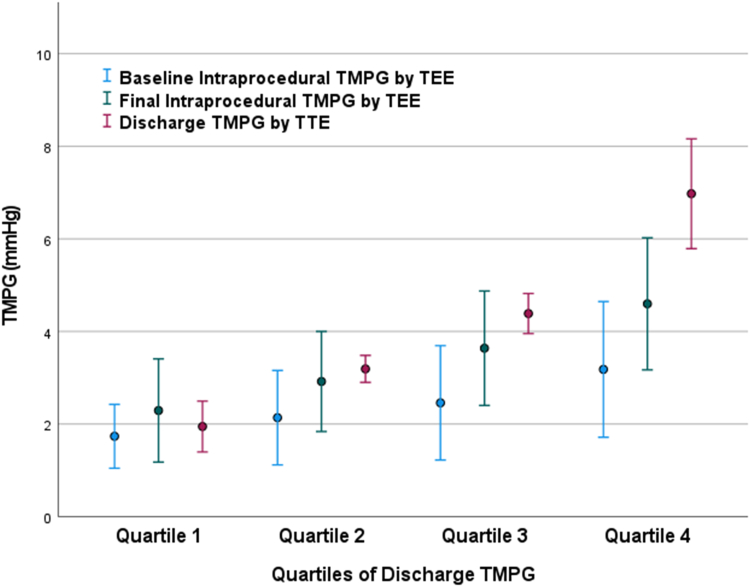
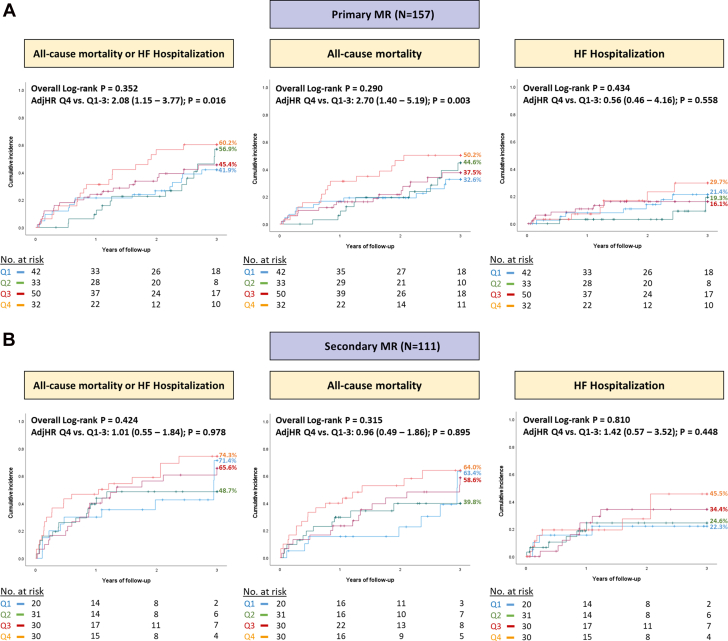
Methods: Consecutive patients undergoing M-TEER at our institution between 2014 and 2022 were included and divided based on quartiles of predischarge TMPG. Outcomes were assessed using Kaplan-Meier analysis and Cox proportional hazard models. We performed subgroup analyses according to mitral regurgitation (MR) mechanism. The primary outcome was all-cause mortality or heart failure hospitalization.
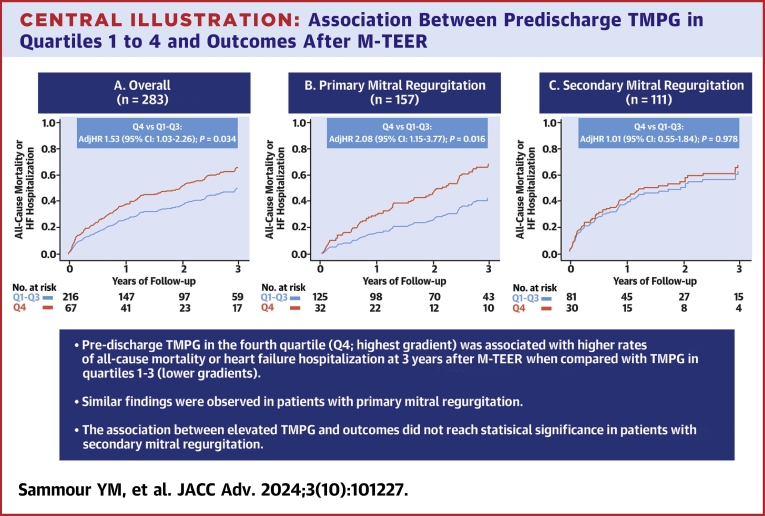
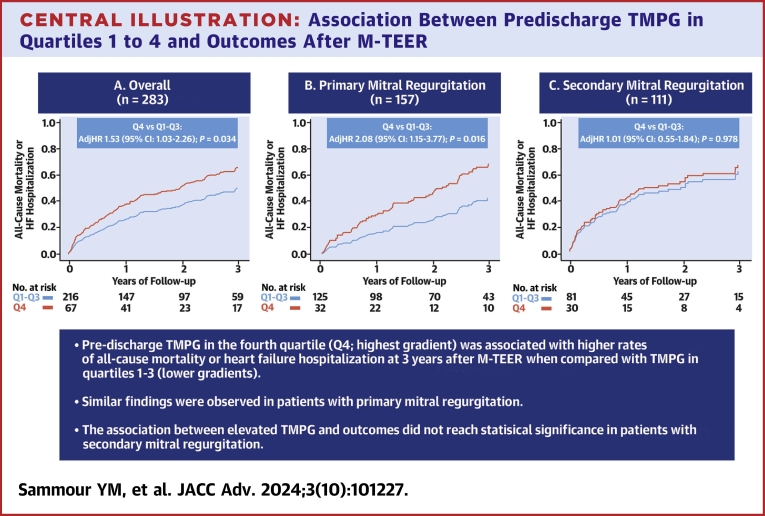
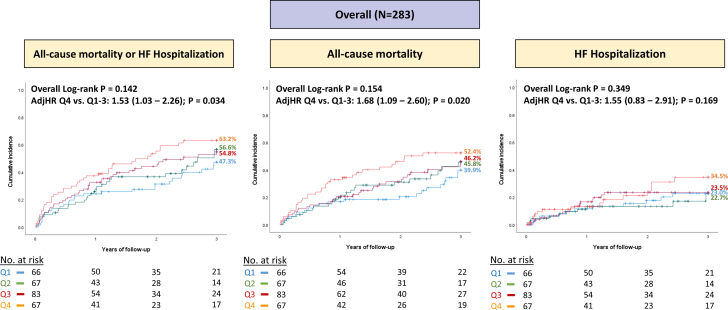
Results: We included 283 patients (age 76.7 ± 10.8 years, 42.8% women, 78.4% Caucasian, and baseline TMPG 2.4 ± 1.3 mm Hg). Higher baseline TMPG was a predictor of increased TMPG after M-TEER (coefficient 0.60 [95% CI: 0.40-0.70]; P < 0.001). In comparison with predischarge TMPG quartiles 1 to 3, those in quartile 4 (7.0 ± 1.1 mm Hg) had an increased risk of 3-year all-cause mortality or heart failure hospitalization (adjHR: 1.53 [95% CI: 1.03-2.26]; P = 0.034), as well as all-cause mortality alone (adjusted HR [adjHR]: 1.68 [95% CI: 1.09-2.60]; P = 0.020). Among patients with primary MR, similar findings were seen for the composite endpoint (adjHR: 2.08 [95% CI: 1.15-3.77]; P = 0.016), and all-cause mortality (adjHR: 2.70 [95% CI: 1.40-5.19]; P = 0.003). However, this association did not reach statistical significance in secondary MR.
Conclusions: In this single-center study, higher residual TMPG after M-TEER was associated with worse outcomes at intermediate- to long-term follow-up. The effect was mainly driven by increased mortality especially in patients with primary MR. Operators should strive to lower residual TMPG before the conclusion of the procedure.
Keywords: MVG; MitraClip; TEER; TMPG; mean gradient; mitral repair; outcomes.
© 2024 The Authors.
Conflict of interest statement
Dr Atkins is a consultant for WL Gore & Associates. Dr Reardon is a consultant for Medtronic, Boston Scientific, Abbott, and WL Gore & Associates. Dr Kleiman is a local principal investigator in trials sponsored by 10.13039/100008497Boston Scientific, 10.13039/100004374Medtronic, 10.13039/100000046Abbott, and 10.13039/100006520Edwards Lifesciences. Dr Goel is a consultant for Medtronic, WL Gore & Associates, and JC Medical; and is on the Speakers Bureau for Abbott Structural Heart. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Feldman T., Foster E., Glower D.D., et al. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011;364:1395–1406. - PubMed
-
- Stone G.W., Lindenfeld J., Abraham W.T., et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med. 2018;379:2307–2318. - PubMed
-
- Hahn R.T., Hausleiter J. Transmitral gradients following transcatheter edge-to-edge repair: are mean gradients meaningful? JACC Cardiovasc Interv. 2022;15:946–949. - PubMed
-
- Koell B., Ludwig S., Weimann J., et al. Long-term outcomes of patients with elevated mitral valve pressure gradient after mitral valve edge-to-edge repair. JACC Cardiovasc Interv. 2022;15:922–934. - PubMed
LinkOut - more resources
Full Text Sources
