

Association between psychopharmacotherapy and postpartum hemorrhage
- PMID: 39512763
- PMCID: PMC11541838
- DOI: 10.1016/j.xagr.2024.100402
Association between psychopharmacotherapy and postpartum hemorrhage
Abstract
Background: Prior studies evaluating the relationship between psychopharmacotherapy (PPT), and postpartum hemorrhage (PPH) have yielded inconsistent findings. Clarifying this potential relationship is important for effective counseling and risk stratification.
Objectives: Our primary objective was to evaluate the association between prenatal exposure to PPT (any drug class) and the occurrence of PPH requiring transfusion of packed red blood cells (PPH+pRBC) after systematically adjusting for known hemorrhage risk factors at the time of admission for delivery. Secondary objectives were to evaluate the association between individual PPT drug classes and PPH+pRBC, and the association between treatment intensity of mental health condition and PPH+pRBC. Finally, we evaluated the association between PPT and a broader definition of PPH that included deliveries requiring multiple uterotonic drugs.
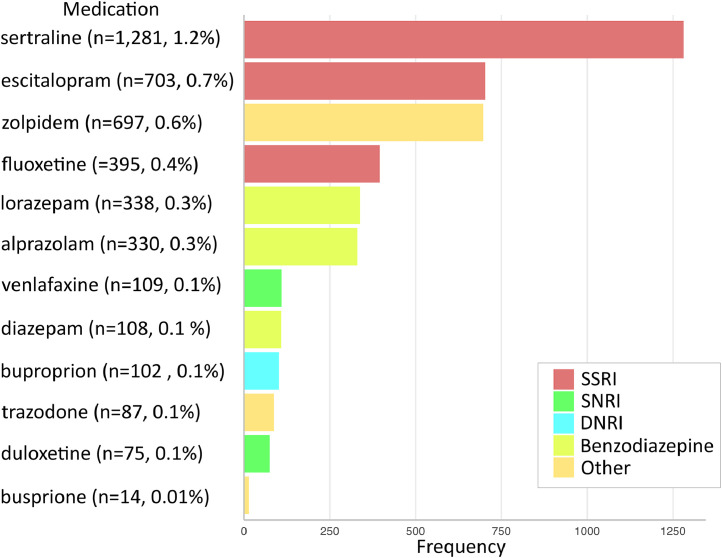
Study design: This is a retrospective cross-sectional study of all pregnancies delivered at 23 weeks of gestational age or greater at seven hospitals within a large academic health system in New York between January 2019 and December 2022. There were no exclusion criteria, as postpartum hemorrhage risk assessment is necessary for all patients admitted for delivery. We assessed exposure to prenatal PPT, including selective serotonin reuptake inhibitors (SSRIs: escitalopram, fluoxetine, sertraline), serotonin-norepinephrine reuptake inhibitors (SNRIs: duloxetine, venlafaxine), dopamine-norepinephrine reuptake inhibitors (DNRIs: buproprion), benzodiazepines (alprazolam, diazepam, lorazepam), and others (buspirone, trazodone, zolpidem). Multivariable logistic regression was performed to evaluate the relationship between PPT and PPH+pRBC, while systematically adjusting for known hemorrhage risk factors at the time of hospital admission. Similar regression analyses were performed to address the secondary objectives.
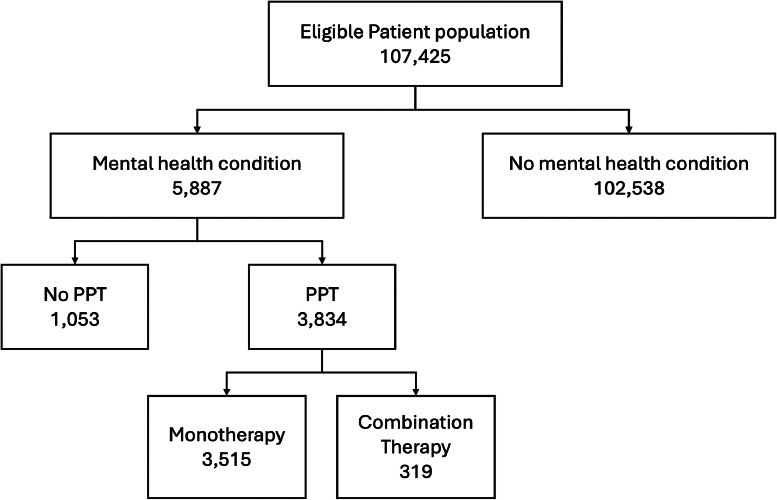
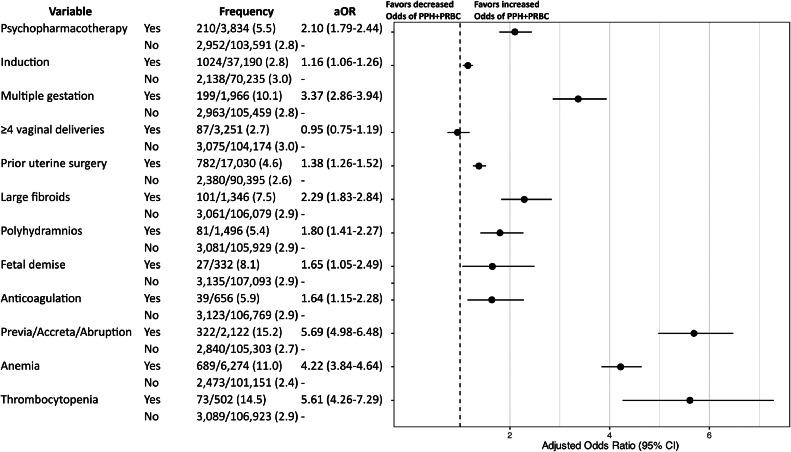
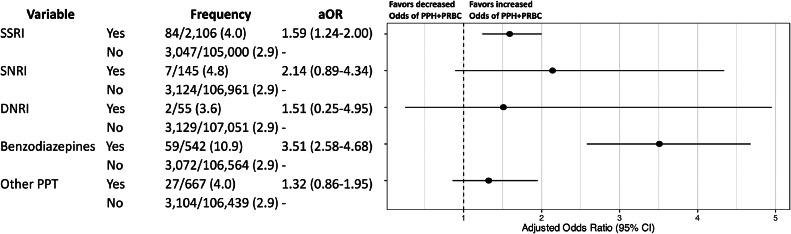
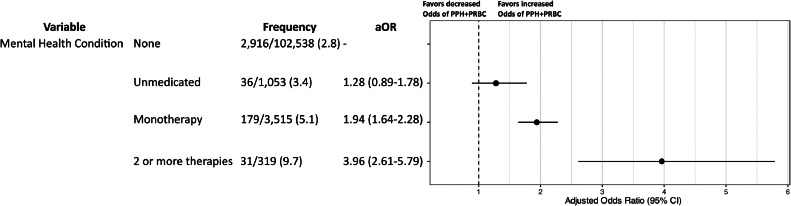
Results: A total of 107,425 deliveries were included. Non-Hispanic White patients constituted the largest race and ethnicity group (43.4%), followed by Hispanic patients (18.7%), Asian or Pacific Islander patients (13.2%), and non-Hispanic Black patients (12.3%). Prenatal exposure to PPT occurred in 3.6% of pregnancies (n=3,834). The overall rate of PPH+pRBC was 2.9% (n=3,162). PPH+pRBC occurred more frequently in pregnancies exposed to PPT than in pregnancies which were not exposed (5.5% vs. 2.8%, respectively; aOR 2.10, 95% CI: 1.79-2.44). SSRIs and benzodiazepine monotherapy were each associated with higher odds of PPH+pRBC than nonexposure. Compared to patients without a mental health condition, monotherapy was associated with nearly 2-fold increased odds and combination PPT was associated with nearly 4-fold greater odds of PPH+pRBC after adjustment for confounding variables (monotherapy: aOR 1.94, 95% CI: 1.64-2.28; combination PPT: aOR 3.96, 95% CI: 2.61-5.79). Patients with untreated mental health conditions (no PTT) had no increased odds of PPH+pRBC compared to those without mental health conditions. Finally, after adjusting for covariates, a positive association was found between PPT and PPH requiring pRBC transfusion and/or the use of two additional uterotonic agents beyond routine postpartum oxytocin (aOR 1.53, 95% CI: 1.35-1.73).
Conclusions: Prenatal PPT exposure is associated with increased odds of clinically significant PPH+pRBC after adjusting for other hemorrhage risk factors. Combination PPT was associated with greater odds of PPH+pRBC than monotherapy.
Keywords: benzodiazepine; bleeding risk assessment; dopamine-norepinephrine reuptake inhibitors; mental health condition; perinatal mood disorder; selective serotonin reuptake inhibitors; serotonin-norepinephrine reuptake inhibitors.
© 2024 The Authors.
Figures
References
LinkOut - more resources
Full Text Sources
