

Tremor in cervical dystonia
- PMID: 39512809
- PMCID: PMC11542928
- DOI: 10.3389/dyst.2024.11309
Tremor in cervical dystonia
Abstract
Background: Cervical dystonia (CD) is the most common form of focal dystonia encountered in the clinic. Approximately one-third of CD patients have co-existing tremor in the head and hands. Assessment of tremor as regular or irregular in context of its oscillation trajectory, frequency, and amplitude is a major clinical challenge and can confound the diagnosis of CD. The misdiagnosis may lead to therapeutic failures, poor quality of life, and poor utilization of medical and financial resources.
Methods: We analyzed the largest cohort of CD patients (n = 3117) available to date, collected from 37 movement disorder centers in North America, Europe, and Asia. We used machine learning to determine what clinical features from clinician reports predicted the presence of tremor as well as its regular or irregular appearance.
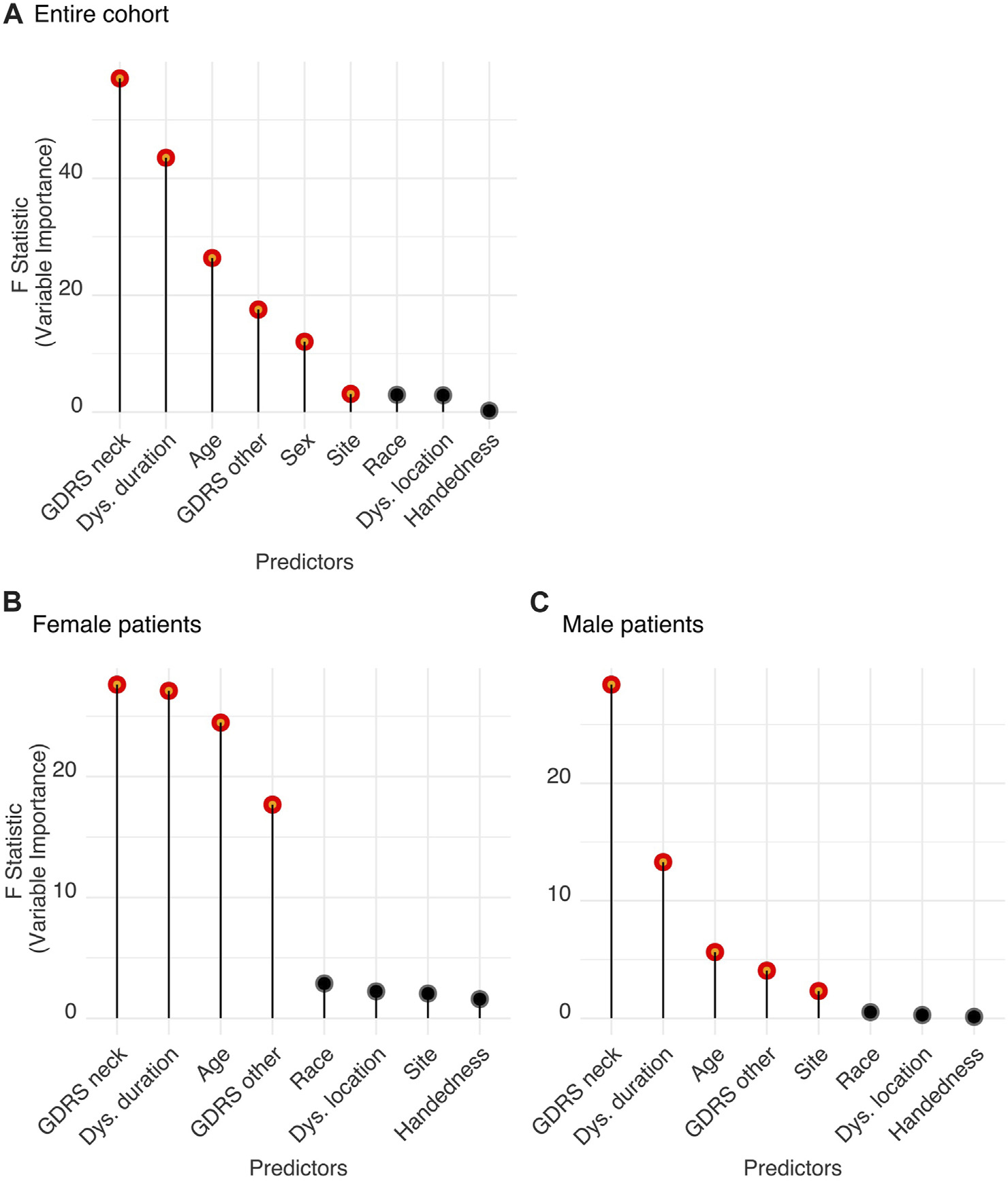
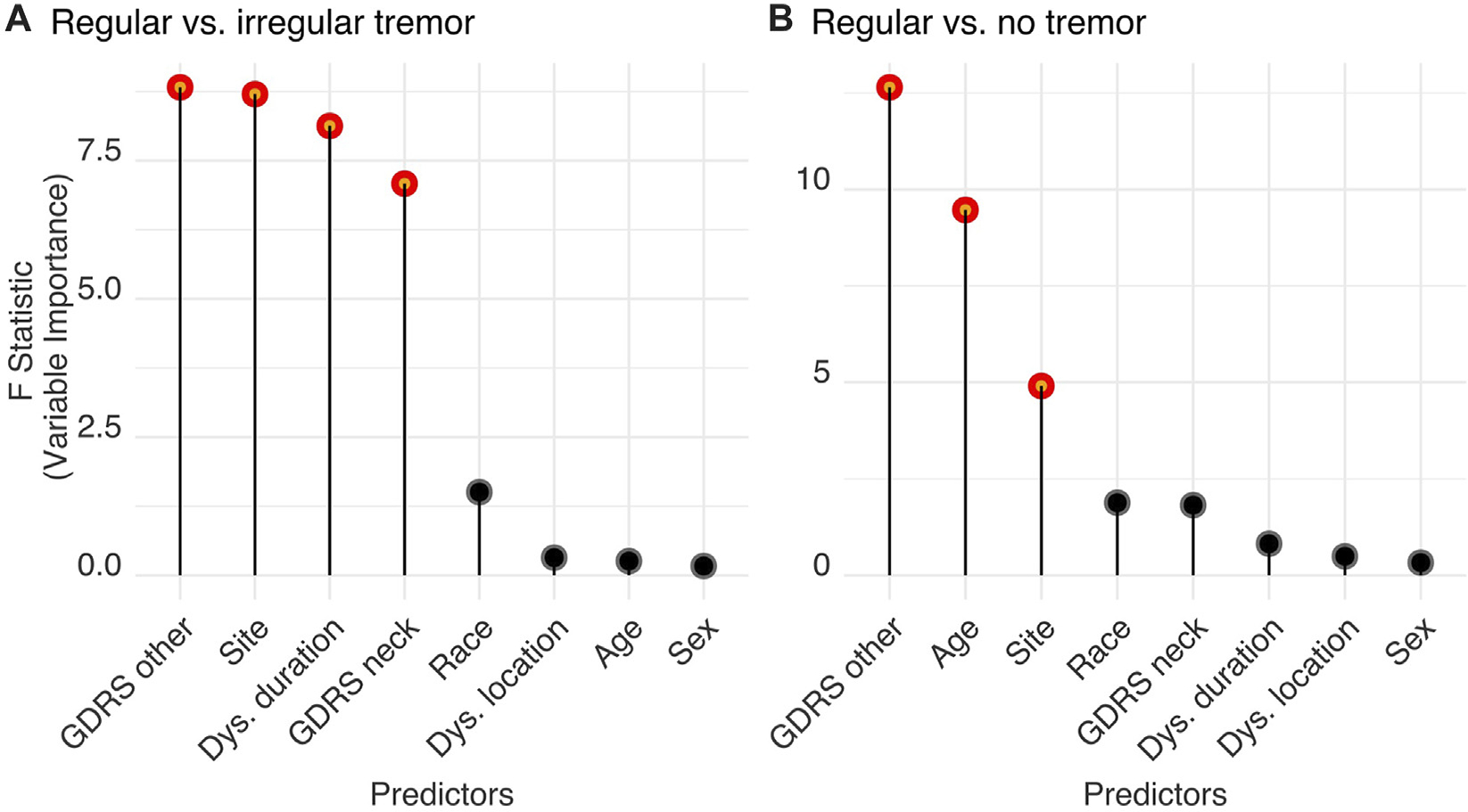
Results: Out of 3,117 CD patients, 1,367 had neck tremor. The neck tremor was interpreted as irregular in 1,022, regular in 345, and mixed (both irregular and regular) in 442. A feature importance analysis determined that greater severity of CD, longer disease duration, and older age, in descending order, predicted the presence of neck tremor. The probability of neck tremor was reduced if the dystonia affected other body parts in addition to the neck. We also found a significantly heightened risk for developing neck tremor in women. An additional feature importance analysis indicated that increased severity of dystonia affecting other body parts, severity of CD, and prolonged disease duration was associated with a lower likelihood of regular neck tremor while increased age predicted a higher likelihood.
Conclusion: Machine learning recognized the most relevant clinical features that can predict concurrent neck tremor and its irregularity in a large multi-center dystonia cohort. These results may facilitate a more accurate description of neck tremor and improved care path in CD.
Keywords: cervical dystonia; dystonia; jerkiness; reularity; tremor.
Conflict of interest statement
Conflict of interest The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources