

Transforming respiratory diseases management: a CMO-based hospital pharmaceutical care model
- PMID: 39512818
- PMCID: PMC11540901
- DOI: 10.3389/fphar.2024.1461473
Transforming respiratory diseases management: a CMO-based hospital pharmaceutical care model
Abstract
Introduction: Respiratory diseases encompass a diverse range of conditions that significantly impact global morbidity and mortality. While common diseases like asthma and COPD exhibit moderate symptoms, less prevalent conditions such as pulmonary hypertension and cystic fibrosis profoundly affect quality of life and mortality. The prevalence of these diseases has surged by approximately 40% over the past 3 decades. Despite advancements in pharmacotherapy, challenges in drug administration, adherence, and adverse effects persist. This study aimed to develop and perform an interim validation of a Capacity-Motivation-Opportunity (CMO) model tailored for respiratory outpatients to enhance pharmaceutical care, which is the direct, responsible provision of medication-related care for the purpose of achieving definite outcomes that improve a patient's quality of life, and overall wellbeing.
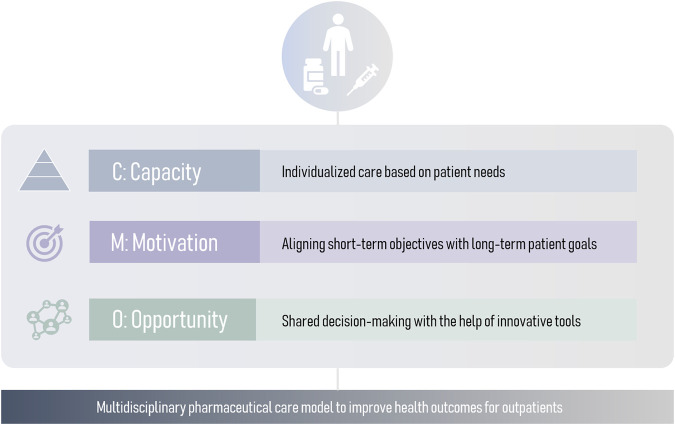
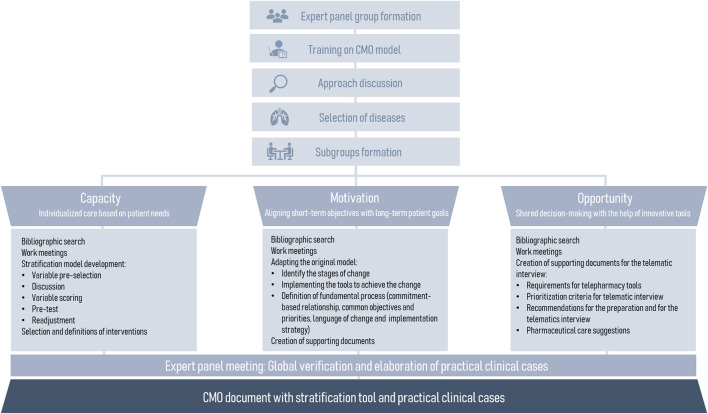
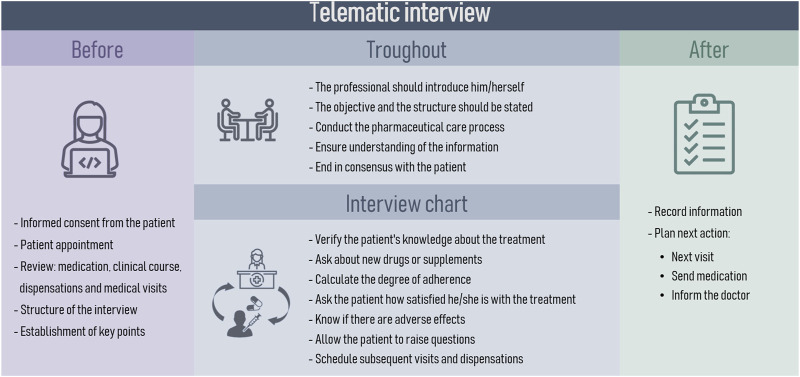
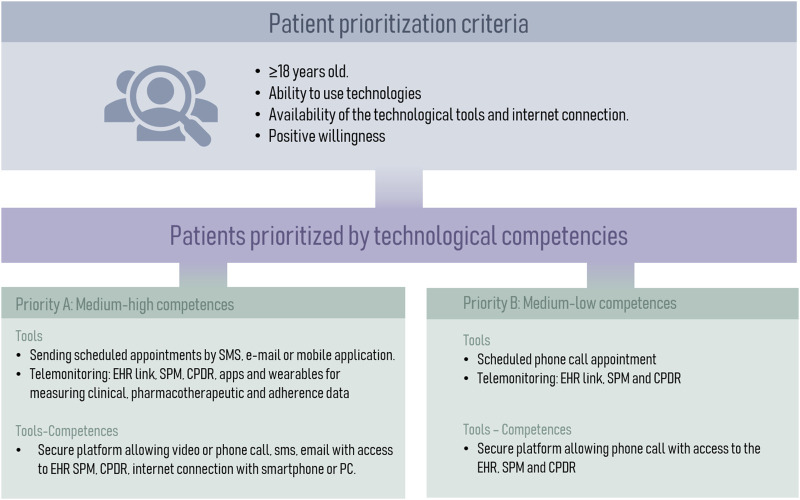
Methodology: This cross-sectional, multicenter study was conducted from March 2022 to March 2023. It comprised four phases: 1) forming an expert panel of 15 hospital pharmacists, 2) selecting respiratory pathologies based on prevalence and severity, 3) developing the CMO model's pillars, and 4) integrating and conducting an interim validation of the model. The Capacity pillar focused on patient stratification and personalized care; the Motivation pillar aligned therapeutic goals through motivational interviewing; and the Opportunity pillar promoted the use of information and communication technologies (ICTs) for telemedicine.
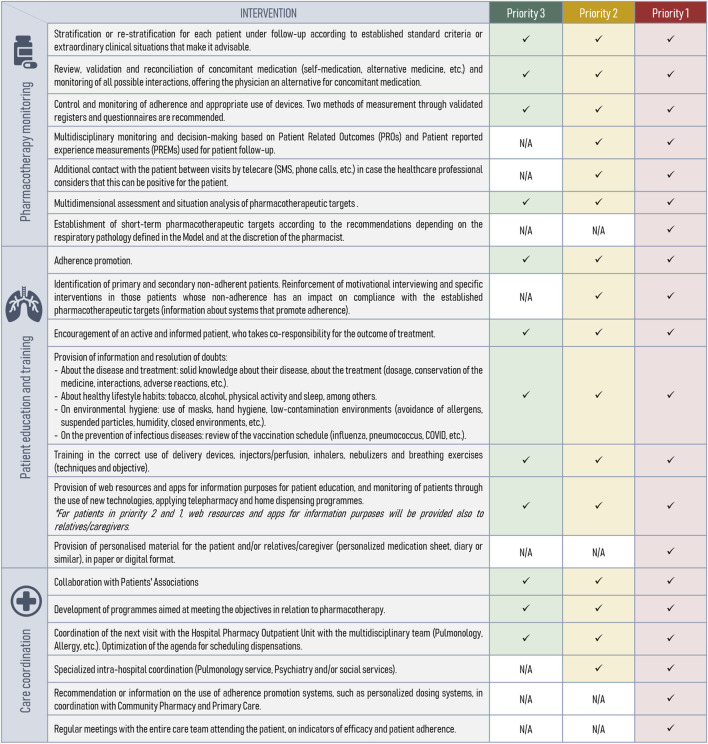
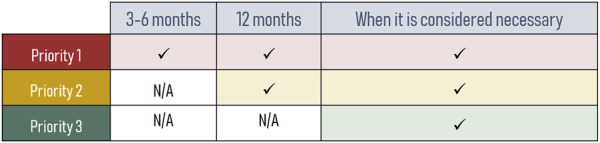
Results: The model included eight respiratory diseases based on expert assessment. For the Capacity pillar, 22 variables were defined for patient stratification, leading to three priority levels for personalized pharmaceutical care. In a preliminary test involving 201 patients across six hospitals, the stratification tool effectively classified patients according to their needs. The Motivation pillar adapted motivational interviewing techniques to support patient adherence and behavior change. The Opportunity pillar established teleconsultation protocols and ICT tools to enhance patient monitoring and care coordination.
Conclusion: The CMO model, tailored for respiratory patients, provides a comprehensive framework for improving pharmaceutical care. By focusing on patient-centered care, aligning therapeutic goals, and leveraging technology, this model addresses the multifaceted needs of individuals with respiratory conditions. Future studies are necessary to validate this model in other healthcare systems and ensure its broad applicability.
Keywords: adherence; behavior; hospital pharmacy; innovation; pharmaceutical care; respiratory diseases.
Copyright © 2024 Zarate-Tamames, Garin, Calvin-Lamas, Jornet, Martinez-Simon, Garcia-Gil, Garcia-Rebolledo and Morillo-Verdugo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
[Comparison of quality of life in patients living with HIV infection through pharmaceutical care according to CMO methodology vs. conventional follow-up. MAS-VIH project].Rev Esp Quimioter. 2024 Apr;37(2):149-157. doi: 10.37201/req/105.2023. Epub 2024 Jan 19. Rev Esp Quimioter. 2024. PMID: 38240196 Free PMC article. Clinical Trial. Spanish.
-
The patient experience of patient-centered communication with nurses in the hospital setting: a qualitative systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):76-87. doi: 10.11124/jbisrir-2015-1072. JBI Database System Rev Implement Rep. 2015. PMID: 26447009
-
A new definition and refocus of pharmaceutical care: the Barbate Document.Farm Hosp. 2020 Jul 1;44(4):158-162. doi: 10.7399/fh.11389. Farm Hosp. 2020. PMID: 32646347 Review. English.
-
Development of a taxonomy for pharmaceutical interventions in HIV+ patients based on the CMO model.Farm Hosp. 2016 Nov 1;40(n06):544-568. doi: 10.7399/fh.2016.40.6.10567. Farm Hosp. 2016. PMID: 27894228 Review. English.
Cited by
-
Comparison of perceived versus actual care complexity in HIV-positive patients receiving antiretroviral treatment: The STRATPATIENT study.Rev Esp Quimioter. 2025 May 27;38(4):278-286. doi: 10.37201/req/014.2025. Epub 2025 May 27. Rev Esp Quimioter. 2025. PMID: 40432448 Free PMC article.
References
-
- Almahdi F. B., Hashim A. H., Albaba E. A. M., Salih O. N., Alkasam R. J., Mosli M. H., et al. (2020). The impact of the pharmaceutical care management model of hepatitis C medications on the cost at health insurance level. Value Health Reg. Issues 21, 230–237. 10.1016/j.vhri.2020.01.004 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous