

Covered stent implantation for calcified nodule to physically hinder its protrusion causing restenosis: a case report
- PMID: 39513136
- PMCID: PMC11538835
- DOI: 10.21037/cdt-24-216
Covered stent implantation for calcified nodule to physically hinder its protrusion causing restenosis: a case report
Abstract
Background: Calcified nodule (CN) is a phenotypic feature of calcified plaques which causes acute coronary syndrome (ACS). Recent studies reported that culprit lesions harboring CN has been shown to increase a risk of repeat revascularization after percutaneous coronary intervention (PCI) with the implantation of newer-generation drug-eluting stent (DES) or debulking device. Mechanistically, a re-protrusion of CN into the lumen has been considered as an important cause associated with repeat revascularization after PCI. These observations suggest the need for additional therapeutic approach to mitigate a risk of repeat revascularization at CN lesions. Here we report a case who received the implantation of one covered stent due to coronary artery perforation after stent implantation at coronary lesion exhibiting CN. This case is unique in terms of preventing restenosis by using covered stent which could physically hinder protrusion of CN through the stent strut.
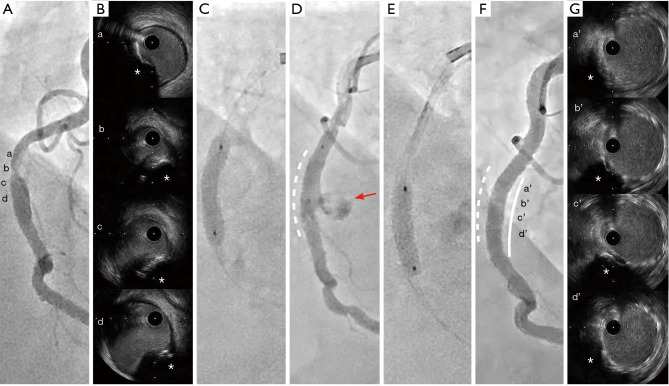
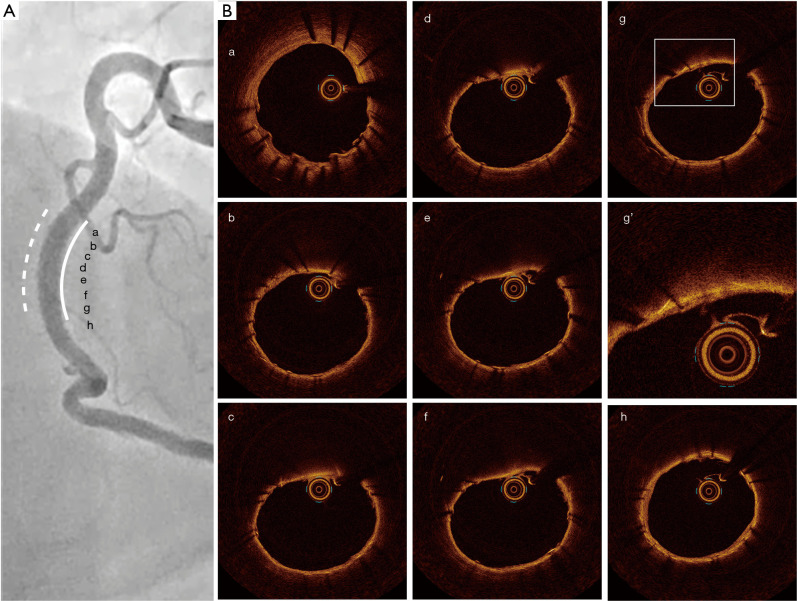
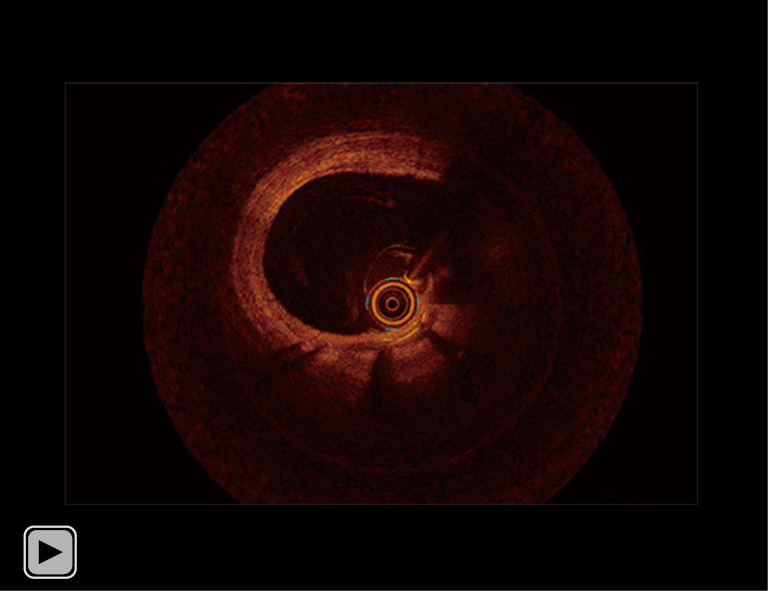
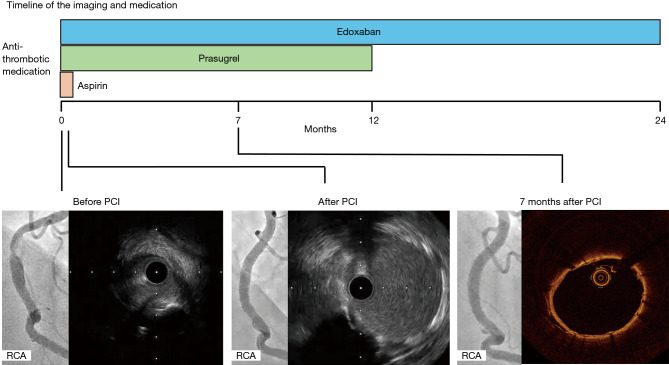
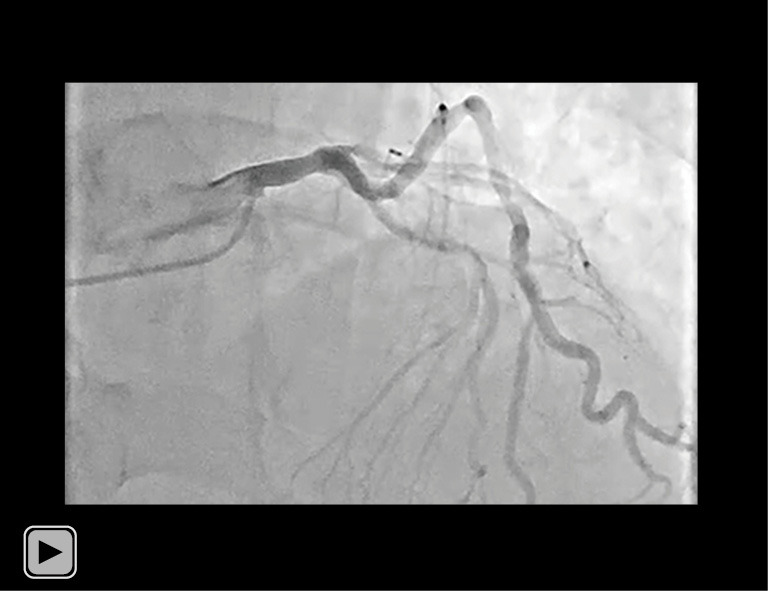
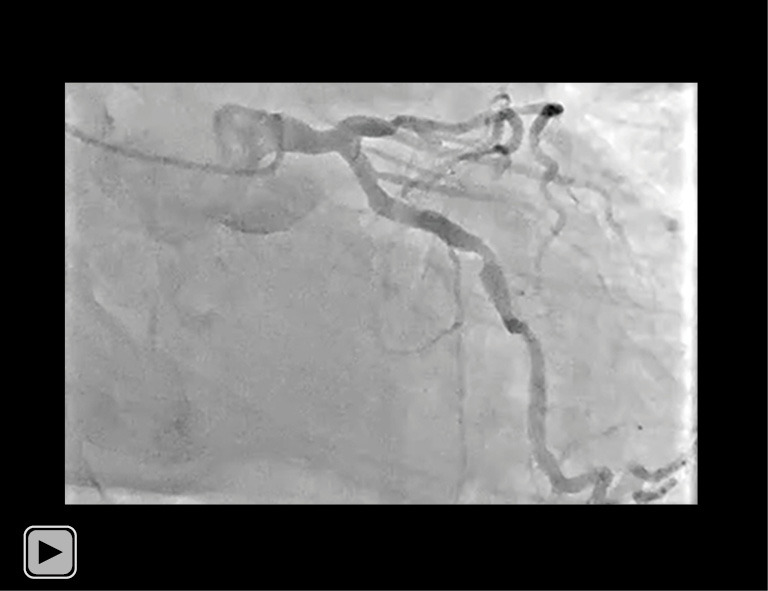
Case description: A 79-year-old man presented to the emergency department with his prolonged chest pain. Although he had a history of hypertension and adrenal hypertrophy, he was not taking any medication prior to his admission. He was diagnosed as ST-segment elevation myocardial infarction. Emergent coronary angiography revealed one severe stenosis in the middle segment of his right coronary artery (RCA). Primary PCI was performed under the guidance of intravascular ultrasound (IVUS) imaging. IVUS imaging prior to PCI revealed a protruding shape of calcification and its irregular surface at his culprit lesion, suggesting the presence of a CN. Following one DES implantation, coronary artery perforation occurred at the segment receiving DES implantation. We implanted one covered stent for the coronary artery perforation. This procedure resulted in successfully sealing coronary artery perforation. Seven months later, follow-up coronary angiography and optical coherence tomography (OCT) imaging were conducted to evaluate his RCA. Any in-stent restenosis (ISR) was not observed. Furthermore, OCT imaging elucidated a small amount of neointimal proliferation without any re-protruding feature of CN through the segment receiving a covered stent. Of note, he did not experience any clinically-driven target lesion revascularization (TLR) for 2 years after PCI.
Conclusions: Our case indicates the use of covered stent as an effective approach to physically hinder the re-protrusion of calcification tissues into the lumen, potentially mitigating a risk of ISR.
Keywords: Calcified nodule (CN); acute coronary syndrome (ACS); case report; covered stent; in-stent restenosis (ISR).
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://cdt.amegroups.com/article/view/10.21037/cdt-24-216/coif). Y.K. serves as an unpaid editorial board member of Cardiovascular Diagnosis and Therapy from September 2023 to August 2025. Y.K. has received research support from Kowa, Nipro and Abbott, and honoraria from Nipro, Abbott, Kowa, Amgen, Sanofi, Astellas, Takeda and Daiichi-Sankyo. The other authors have no conflicts of interest to declare.
Figures
References
-
- Watanabe Y, Sakakura K, Taniguchi Y, et al. Comparison of clinical outcomes of intravascular ultrasound-calcified nodule between percutaneous coronary intervention with versus without rotational atherectomy in a propensity-score matched analysis. PLoS One 2020;15:e0241836. 10.1371/journal.pone.0241836 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous