

Pediatric kidney transplantation in Europe, a clinical snapshot pilot
- PMID: 39513158
- PMCID: PMC11540619
- DOI: 10.3389/fped.2024.1432027
Pediatric kidney transplantation in Europe, a clinical snapshot pilot
Abstract
Background: Pediatric kidney transplantations are rarely performed, and there is limited knowledge about the diversity in current clinical practices across Europe. This study aims to explore the utility of clinical snapshot studies in identifying these disparities, establishing a foundation for future snapshot studies and standardization efforts.
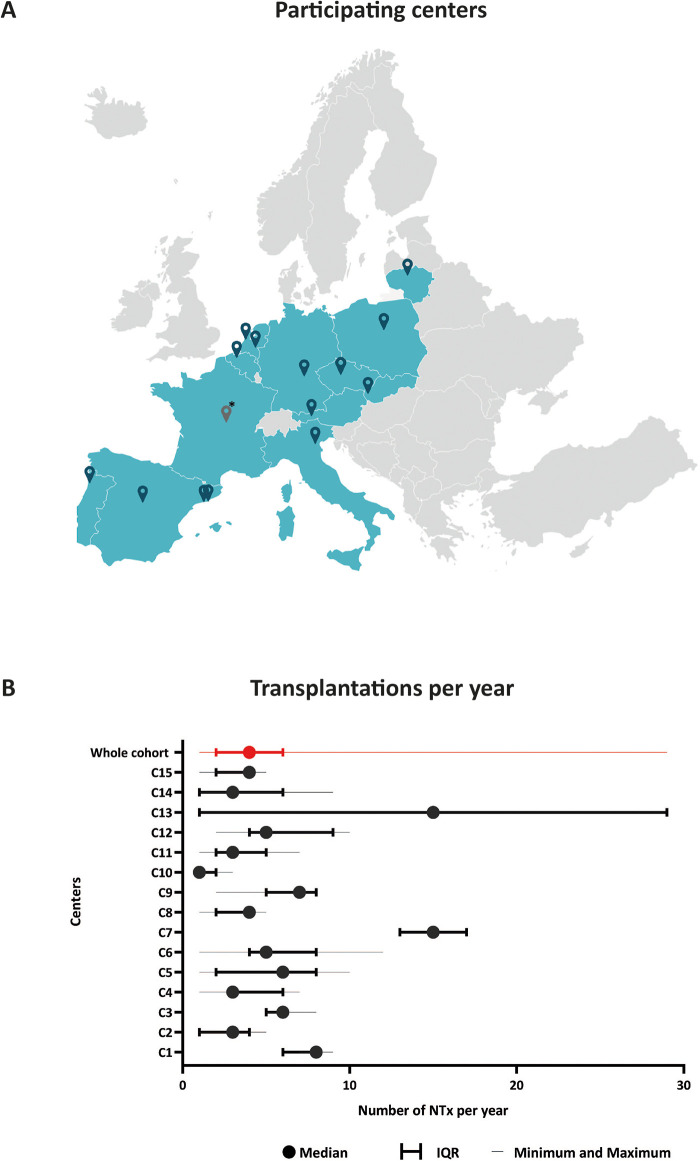
Methods: A pilot clinical snapshot study was conducted, with invitations extended to all 109 pediatric kidney transplant centres in Europe. Each participating centre provided pre-, peri-, and postoperative data concerning their most recent thirty transplantations. The primary outcomes encompassed the evaluation of disparities in donor-recipient selection, surgical techniques, post-operative drainage procedures, and immunosuppressive therapy protocols. Secondary outcomes involved the analysis of rejection rates, incidence of infections, and graft survival.
Results: The study involved 439 patients from fifteen centres (14%) in twelve countries, with varying transplant volumes (range 1-29 transplantations per year) and follow-up periods. Significant differences were found among centres in terms of donor types, cold and warm ischemia time, pre-emptive transplant rates, and kidney transplant drainage methods. The rate of living donors varied between 3% and 90% and the median duration of cold ischemia ranged was 770 min after deceased donation and 147 min after living donation. Basiliximab was the dominant induction therapy, yet steroid withdrawal varied widely. Infection, rejection, and graft survival rates also varied significantly between centres.
Conclusion: This study revealed substantial variation in clinical practices among European centres performing pediatric kidney transplantations. These findings could serve as a stimulus for international dialogue and collaboration.
Keywords: Europe; clinical practice snapshot; donor type; graft survival; pediatric kidney transplantation; registries.
© 2024 Oomen L, Bootsma-Robroeks, Bouts, Carbonell Pradas, Gander, Kienzl-Wagner, König, Pereira, Dunand, Mosca, Pac, Podracka, Prytula, Sangermano, Vitkevic, Zieg, van der Zanden, Feitz and de Wall.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
LinkOut - more resources
Full Text Sources