

The effect of prescription and over-the-counter medications on core temperature in adults during heat stress: a systematic review and meta-analysis
- PMID: 39513185
- PMCID: PMC11541675
- DOI: 10.1016/j.eclinm.2024.102886
The effect of prescription and over-the-counter medications on core temperature in adults during heat stress: a systematic review and meta-analysis
Abstract
Background: Heat stress impacts are an escalating global health concern. Public health bodies such as the World Health Organization (WHO) warn that certain medications impair thermoregulation, with limited supporting evidence. Our aim was to investigate whether medications listed by the WHO increase core temperature responses during heat stress.
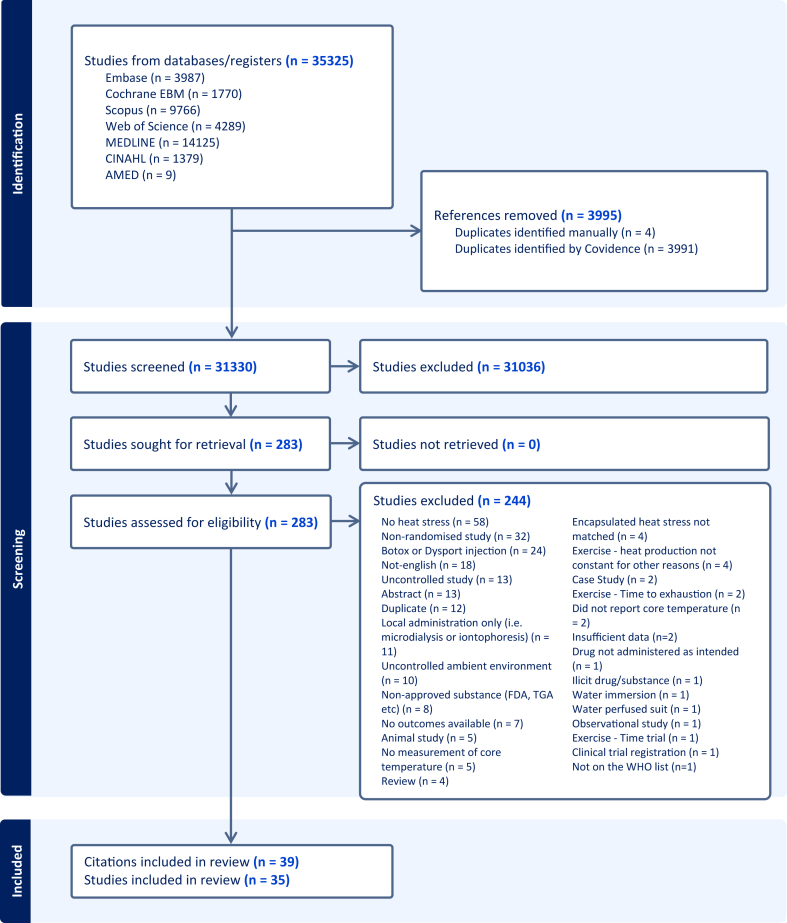
Methods: For this systematic review and meta-analysis, MEDLINE, PubMed, Scopus, CINAHL, Web of Science, and EMBASE were searched up to Jan.30, 2024. Randomised studies exposing humans to exertional and/or passive heat stress that investigated a drug identified by WHO compared to no drug/placebo were eligible. The primary outcome was core temperature (e.g., rectal, oesophageal, aural, tympanic). We assessed risk of bias (Cochrane's Risk of Bias 2) and certainty of evidence (GRADE). The study was pre-registered on PROSPERO (CRD42020170684).
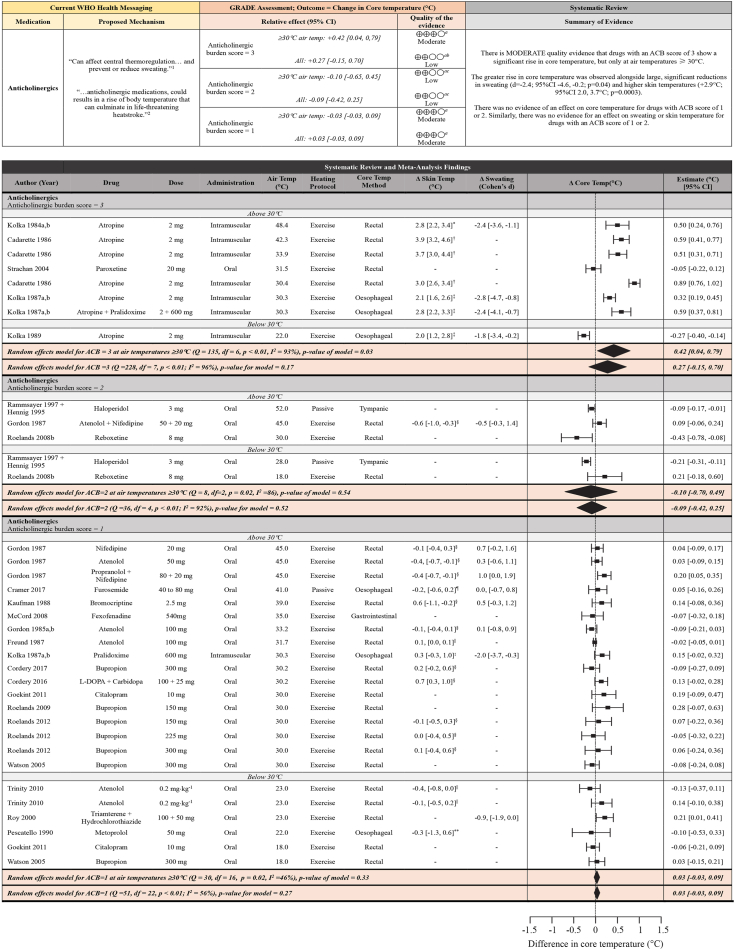
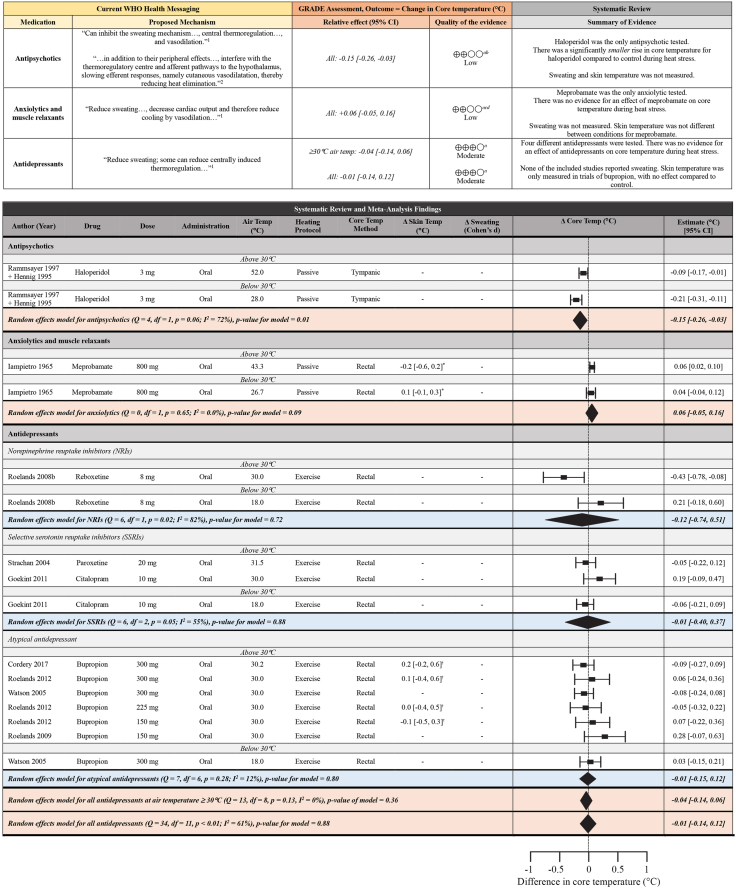
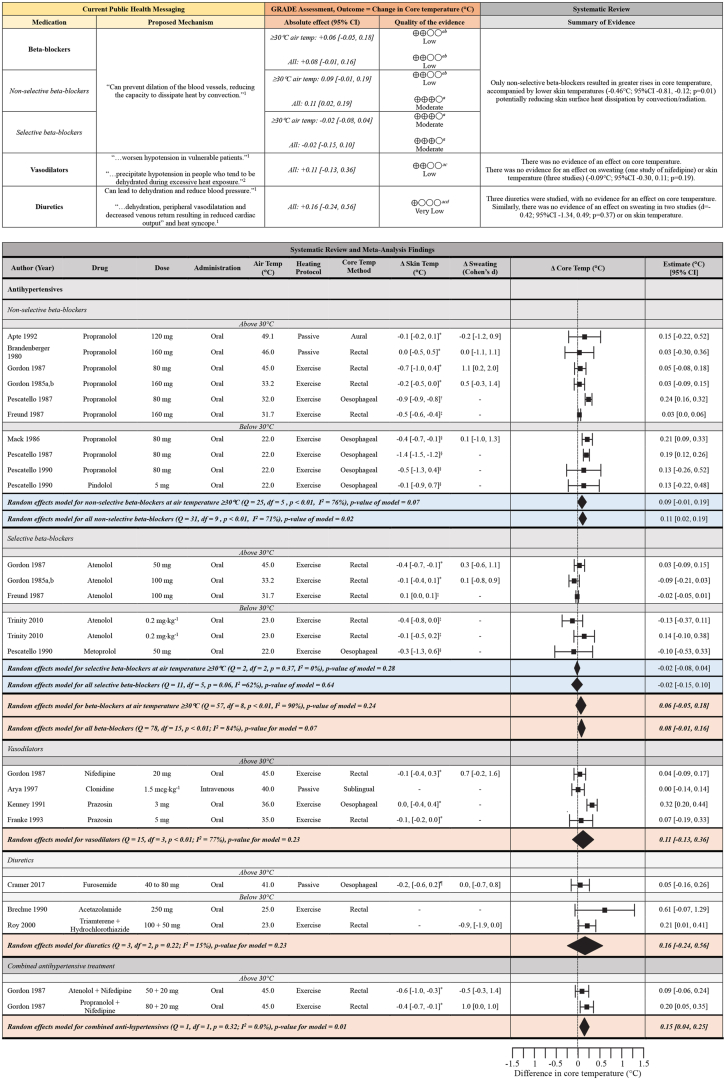
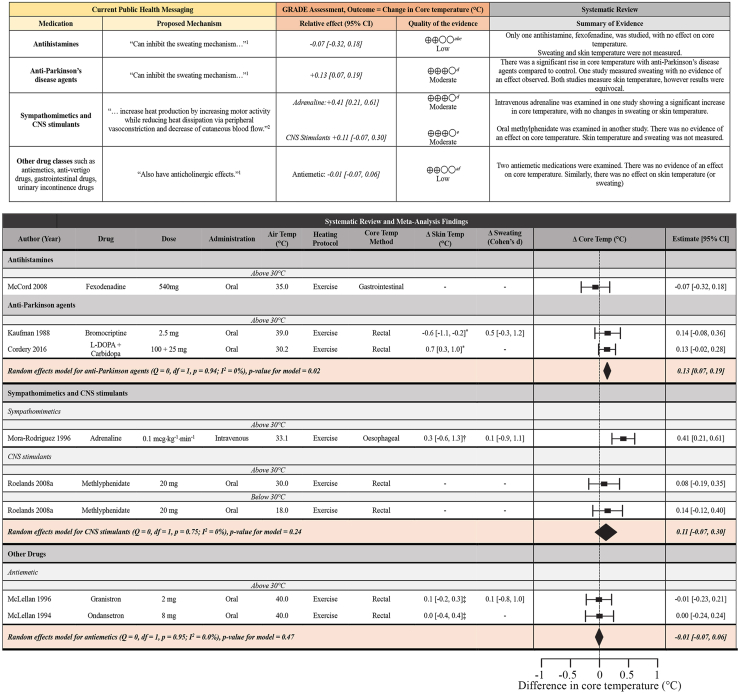
Findings: Thirty-five studies were included enrolling 353 individuals (16 women; 4.5%). Twenty-seven unique medications were tested. The average age of participants across studies was <30 years, and only one study included a clinical population. Under heat stress, there was moderate quality evidence that drugs with high anticholinergic properties increased core temperature at air temperatures ≥30°C (+0.42°C; 95% CI 0.04, 0.79°C; p = 0.03) alongside reduced sweating, although evidence is limited to the drug atropine. Similarly, non-selective beta-blockers (+0.11°C; 95% CI 0.02, 0.19°C; p = 0.02), adrenaline (+0.41°C; 95% CI 0.21, 0.61°C) and anti-Parkinson's agents (+0.13°C; 95% CI 0.07, 0.19°C; p = 0.02) elevated core temperature. Antidepressants, diuretics, or drugs with weak anticholinergic effects did not alter core temperature responses.
Interpretation: Current evidence supports strong anticholinergics, non-selective beta-blockers, adrenaline, and anti-Parkinson's agents impairing thermoregulation during heat stress. No evidence indicated thermoregulation is impacted by other WHO-listed medications. Evidence is predominantly limited to healthy young men, with short heat stress exposures. Studies over longer durations, in women, older adults and those with chronic diseases are required to better inform the pharmaceutical management of patients during hot weather.
Funding: This study was supported by a National Health and Medical Research Council (NHMRC) Investigator Grant (2021/GNT2009507; Holder: O. Jay).
Keywords: Drugs; Heat illness; Medications; Thermoregulation.
© 2024 The Author(s).
Conflict of interest statement
KLB reports grants from the NIH, Wellcome Trust, honoraria for keynote talks and travel support from the World Health Organization to attend meetings, conferences and give keynote talks. KLB is also the Chair of the US National Academy of Sciences Board on Environmental Change and Society. All of KLBs declarations are outside the scope of the submitted work. LK acknowledges funding from the National Institutes of Health (NIH; AG067471) outside of the submitted work. OJ acknowledges funding from the National Health and Medical Research Council (NHMRC 2021/GNT2009507) for the submitted work. OJ also reports grants from the Wellcome Trust and Resilience NSW, consulting fees from a National Institutes of Health grant, expert testimony for the National Rugby League, support for attending meetings and travel from the Global Heat and Health Information Network and Minderoo Foundation – all of which are outside the scope of the submitted work.
Figures
References
-
- National Center for Health Statistics . 2019. Health, United States, 2019: Table 039 Prescription drug use in the past 30 days, by sex, race and Hispanic origin, and age: United States, selected years 1988-1994 through 2015-2018. Hyattsville, MD.https://www.cdc.gov/nchs/hus/data-finder.htm Last updated June 26, 2023.
-
- World Health Organization. Regional Office for Europe . World Health Organization. Regional Office for Europe; Copenhagen: 2011. Public health advice on preventing health effects of heat: new and updated information for different audiences.
-
- World Health Organization. Regional Office for Europe . WHO Regional Office for Europe; Copenhagen: 2009. Improving public health responses to extreme weather/heat-waves : EuroHEAT : technical summary.
-
- Centers for Disease Control and Prevention . 2022. Tips for preventing heat-related illness.https://www.cdc.gov/disasters/extremeheat/heattips.html
-
- Health Canada . Health Canada; Ottawa, ON, Canada: 2011. Extreme heat events guidelines: technical guide for health care workers.
LinkOut - more resources
Full Text Sources
