

Systematic review of oral health in slums and non-slum urban settings of Low and Middle-Income Countries (LMICs): Disease prevalence, determinants, perception, and practices
- PMID: 39514587
- PMCID: PMC11548750
- DOI: 10.1371/journal.pone.0309319
Systematic review of oral health in slums and non-slum urban settings of Low and Middle-Income Countries (LMICs): Disease prevalence, determinants, perception, and practices
Abstract
Background: A comprehensive summary of evidence about oral health in slum settings that could inform policy directions is lacking.
Objective: To summarise the latest evidence regarding oral disease burden and their determinants, perceptions, practices, and service utilization in the slums and non-slum urban settings of LMICs.
Design: Systematic review.
Data sources: Embase and MEDLINE (Ovid); PubMed; Scopus, Web of Science, CRD DARE Database; ELDIS; Essential Health Links; HINARI; African Index Medicus (AIM); and Bioline International, all searched from January 2000 to June 2023 using slum-related terms.
Eligibility criteria: Empirical studies of all designs were eligible. Studies published in English with full-text available and reporting disease burden, perceptions, behaviours and service utilisation related to oral health of residents of slums or broader settings including slums in low and middle-income countries were included.
Data extraction, quality assessment, synthesis and reporting: Studies were categorised and data were extracted and charted according to a preliminary conceptual framework refined by emerging findings. The Mixed Methods Assessment Tool (MMAT) was used to appraise the quality of empirical studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and (where applicable) the Synthesis Without Meta-analysis (SWiM) guideline were adopted for guiding synthesis and reporting. Results were tabulated and narratively summarised.
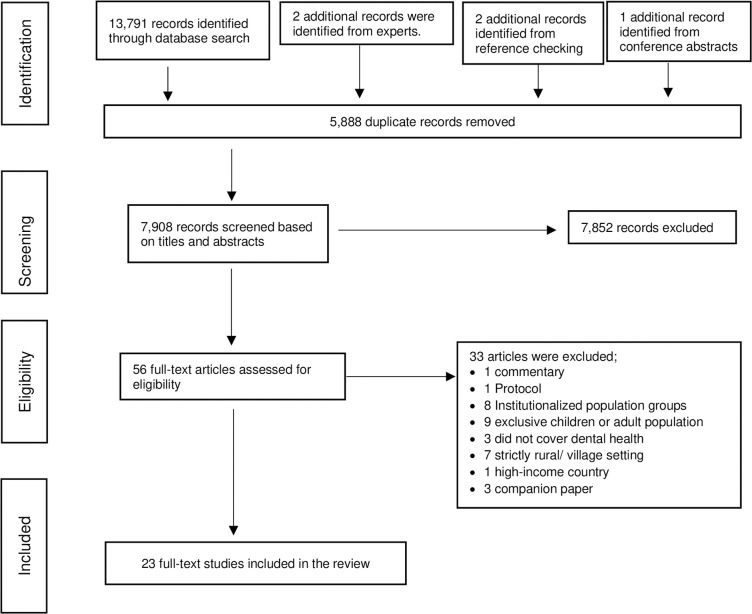
Results: Full-text articles for 56 records were assessed for eligibility and 23 of the articles were included in this review. The majority (13 studies, 57%) were conducted in Asia, and nine studies (39%) in Africa. Six focused on slums (two examined slum and urban non-slum and four examined purely slum settings), two examined general urban settings, eight included both rural and urban areas in their settings, two examined disadvantaged/low socioeconomic, one assessed rural/urban/metropolis/municipal/district, three covered the national population or whole country, and one looked at high versus low socioeconomic regions. The commonest oral diseases reported were dental caries (prevalence: 13% - 76%), and periodontal diseases (prevalence: 23% - 99%). These were higher in slum settings and showed differences across age groups, gender, and socioeconomic classes. Most participants in the studies perceived their oral health status as satisfactory, a belief commoner among younger people, males, those in higher socio-economic classes, and employed. Mouth cleaning was mostly once daily, usually in the mornings. The use of toothpaste and brush was commonest. Other oral hygiene implements included toothpowder, chewing-stick, neem, charcoal, sand, snuff, salt, and the fingers. There was widespread engagement in home remedies for oral disease cure or prevention, while the use of professional dental care facilities was generally low and problem-driven.
Conclusion: The systematic review identified a sparse body of literature on oral health surveys in slums and other urban settings in LMICs. Available data suggest a high oral disease burden, worse in slums, use of inappropriate mouth cleaning tools, self-care practices for pain relief, and few visits to care facilities.
Systematic review registration: Systematic review registration with PROSPERO in February 2020, number CRD42020123613.
Copyright: © 2024 Osuh et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Beyond the black stump: rapid reviews of health research issues affecting regional, rural and remote Australia.Med J Aust. 2020 Dec;213 Suppl 11:S3-S32.e1. doi: 10.5694/mja2.50881. Med J Aust. 2020. PMID: 33314144
-
Nutritional interventions for preventing stunting in children (birth to 59 months) living in urban slums in low- and middle-income countries (LMIC).Cochrane Database Syst Rev. 2019 Jun 17;6(6):CD011695. doi: 10.1002/14651858.CD011695.pub2. Cochrane Database Syst Rev. 2019. PMID: 31204795 Free PMC article.
-
Factors associated with accessing and utilisation of healthcare and provision of health services for residents of slums in low and middle-income countries: a scoping review of recent literature.BMJ Open. 2022 May 24;12(5):e055415. doi: 10.1136/bmjopen-2021-055415. BMJ Open. 2022. PMID: 35613790 Free PMC article.
-
Oral health in an urban slum, Nigeria: residents' perceptions, practices and care-seeking experiences.BMC Oral Health. 2023 Sep 9;23(1):657. doi: 10.1186/s12903-023-03303-5. BMC Oral Health. 2023. PMID: 37689626 Free PMC article.
-
The economics of healthcare access: a scoping review on the economic impact of healthcare access for vulnerable urban populations in low- and middle-income countries.Int J Equity Health. 2022 Dec 31;21(1):191. doi: 10.1186/s12939-022-01804-3. Int J Equity Health. 2022. PMID: 36585704 Free PMC article.
Cited by
-
Oral health awareness, self-care practices, and lived experiences among cancer patients in Ethiopia: a mixed-methods study.BMC Oral Health. 2025 Jun 2;25(1):882. doi: 10.1186/s12903-025-06260-3. BMC Oral Health. 2025. PMID: 40457371 Free PMC article.
-
Factors influencing dental care services utilization in India using Andersen health behaviour model: a systematic review.BMC Health Serv Res. 2025 Jul 29;25(1):988. doi: 10.1186/s12913-025-13252-0. BMC Health Serv Res. 2025. PMID: 40730996 Free PMC article.
-
Does viral circulation in slums have a global impact? The lesson learned from SARS-CoV-2 circulation in Complexo de favelas da Maré, Rio de Janeiro, Brazil.Front Microbiol. 2025 Feb 12;16:1483895. doi: 10.3389/fmicb.2025.1483895. eCollection 2025. Front Microbiol. 2025. PMID: 40012790 Free PMC article.
-
CNN-based remote dental diagnosis model for caries detection with grad-CAM.Sci Rep. 2025 Jul 22;15(1):26555. doi: 10.1038/s41598-025-11447-3. Sci Rep. 2025. PMID: 40695984 Free PMC article.
References
-
- Møller A, Myles P. What makes a good systematic review and meta-analysis? 2016. Oxford University Press. - PubMed
-
- Osuh ME. Prevalence and Determinants of Oral Diseases and Oral Health Care Needs in Slums: A comparative study with non-slum urban settings in Nigeria, in Division of Health Sciences, WMS. 2022. University of Warwick: United Kingdom.
-
- Osuh ME, Oke GA, Lilford RJ, Owoaje E, Harris B, Taiwo OJ, et al.. Prevalence and determinants of oral health conditions and treatment needs among slum and non-slum urban residents: Evidence from Nigeria. PLOS Global Public Health. 2022;2(4):e0000297. doi: 10.1371/journal.pgph.0000297 - DOI - PMC - PubMed
-
- UN-HABITAT. The Challenges of Slums. UN-HABITAT’s new Global Report on Human Settlements. 2003.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
