

Centrally adjudicated vs. investigator-reported outcomes in randomized heart failure trials
- PMID: 39515836
- PMCID: PMC11646619
- DOI: 10.1093/eurheartj/ehae753
Centrally adjudicated vs. investigator-reported outcomes in randomized heart failure trials
Abstract
Background and aims: Heart failure endpoints in cardiovascular outcome trials are commonly identified through centralized adjudication of investigator-reported events. It remains unclear whether central adjudication improves the accuracy of treatment effect estimates in terms of log[hazard ratios (HR)].
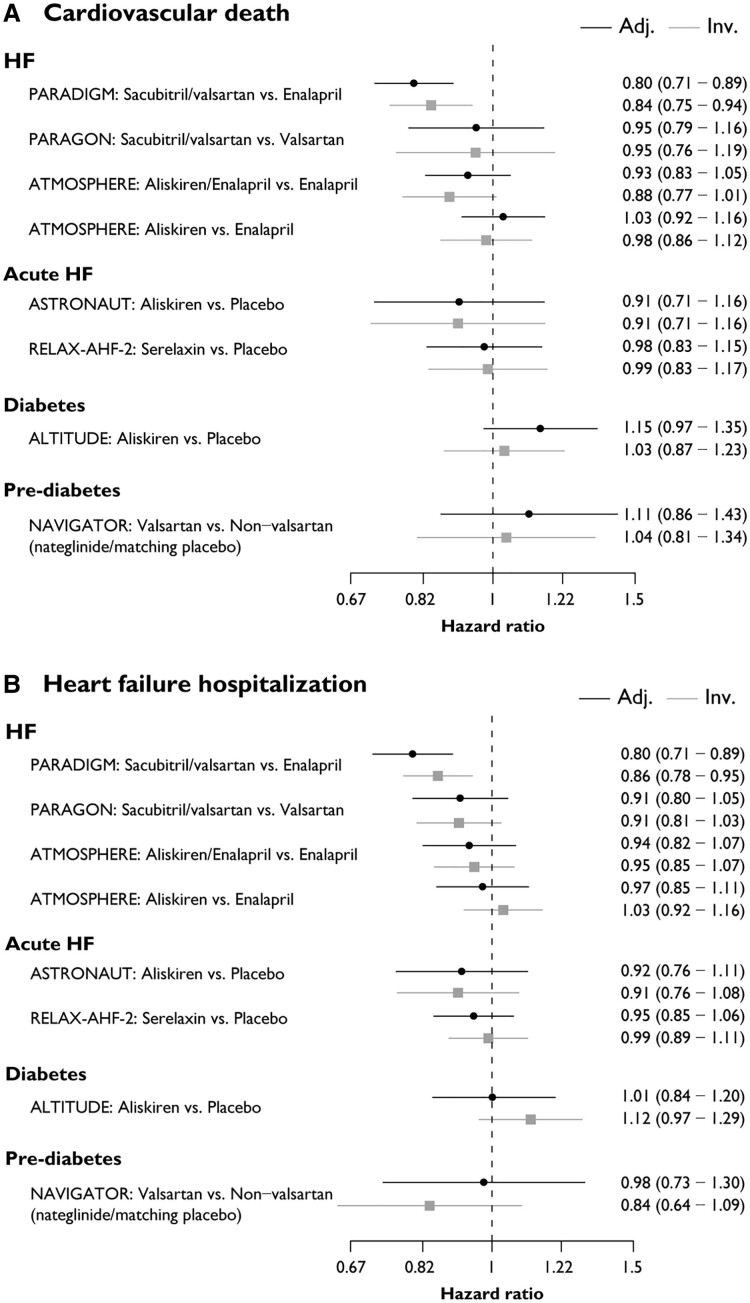
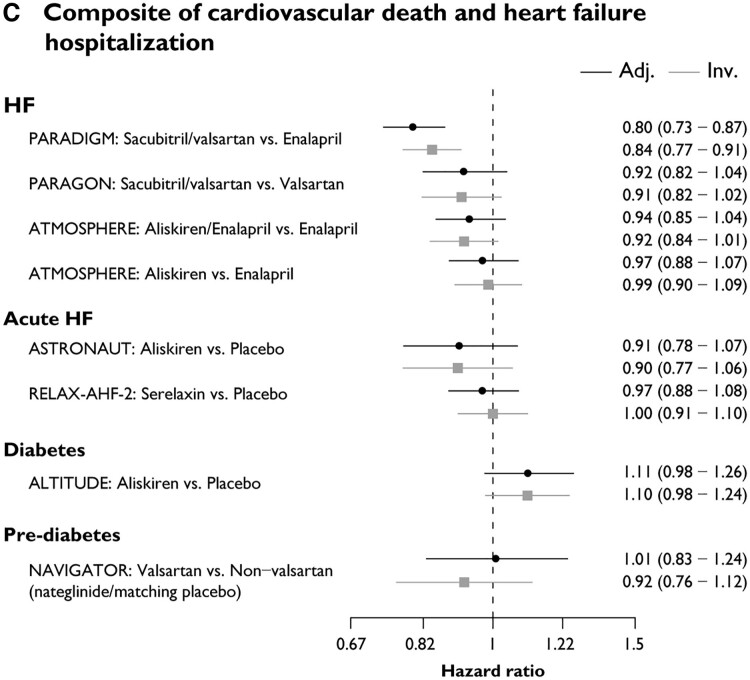
Methods: Data from seven cardiovascular outcome trials with >1000 patients that included centrally adjudicated heart failure outcomes were utilized to assess (i) the concordance between investigator-reported and centrally adjudicated heart failure and cardiovascular death events; (ii) rates of subsequent all-cause mortality following positively vs. negatively adjudicated heart failure events; and (iii) the correlation of log(HR) based on centrally adjudicated vs. investigator-reported events.
Results: Positive adjudication rates for investigator-reported events varied widely across trials, but were generally higher for cardiovascular death (range: 87.9%-99.2%) than for heart failure hospitalization (range: 61.6%-88.0%). The risk for subsequent all-cause death was similar for positively and negatively adjudicated heart failure hospitalizations. Log(HR) correlated well for cardiovascular death [R2 = .80, 95% credible interval (CrI): 0.53-0.93] and the composite of cardiovascular death or heart failure hospitalization (R2 = .79, 95% CrI: 0.46-0.93), but less for heart failure hospitalization (R2 = .57, 95% CrI: 0.10-0.83).
Conclusions: Positive adjudication rates were lower for heart failure events than cardiovascular death, but even negatively adjudicated heart failure events are prognostically important. Central adjudication of events did not alter the results (precision or estimated log(HR)), though some variation was observed, depending on the indication. The results suggest that the decision to pursue centralized adjudication of heart failure events in a specific trial may need to be individualized.
Keywords: Adjudication; Cardiovascular trial; Heart failure; Investigator-reported outcomes.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures



References
-
- Tyl B, Lopez Sendon J, Borer JS, Lopez De Sa E, Lerebours G, Varin C, et al. Comparison of outcome adjudication by investigators and by a central end point committee in heart failure trials: experience of the SHIFT heart failure study. Circ Heart Fail 2020;13:e006720. 10.1161/CIRCHEARTFAILURE.119.006720 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
