

Multi-strain modeling of influenza vaccine effectiveness in older adults and its dependence on antigenic distance
- PMID: 39516205
- PMCID: PMC11549341
- DOI: 10.1038/s41598-024-72716-1
Multi-strain modeling of influenza vaccine effectiveness in older adults and its dependence on antigenic distance
Abstract
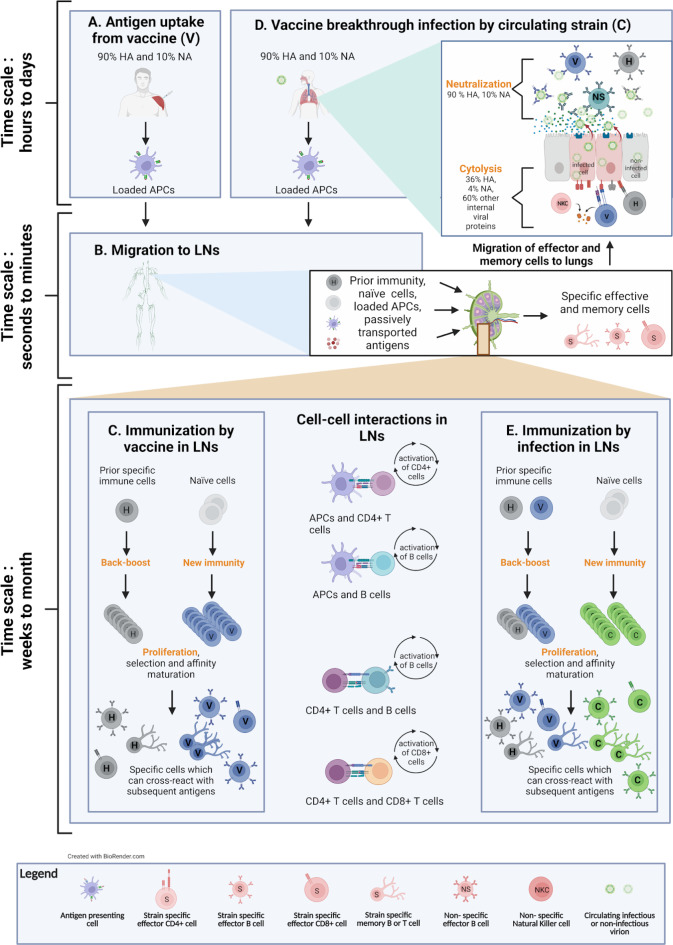
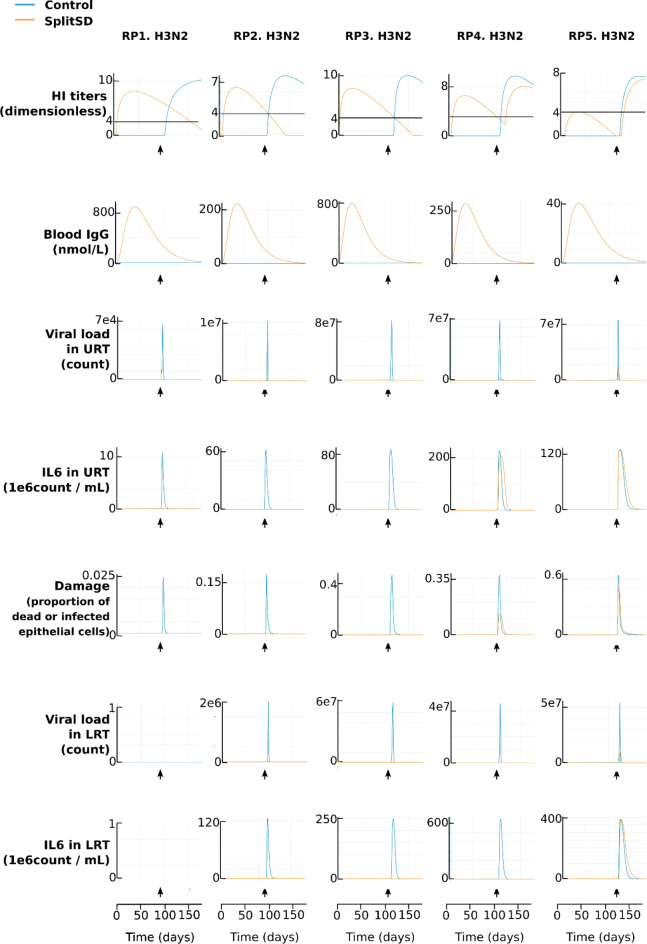
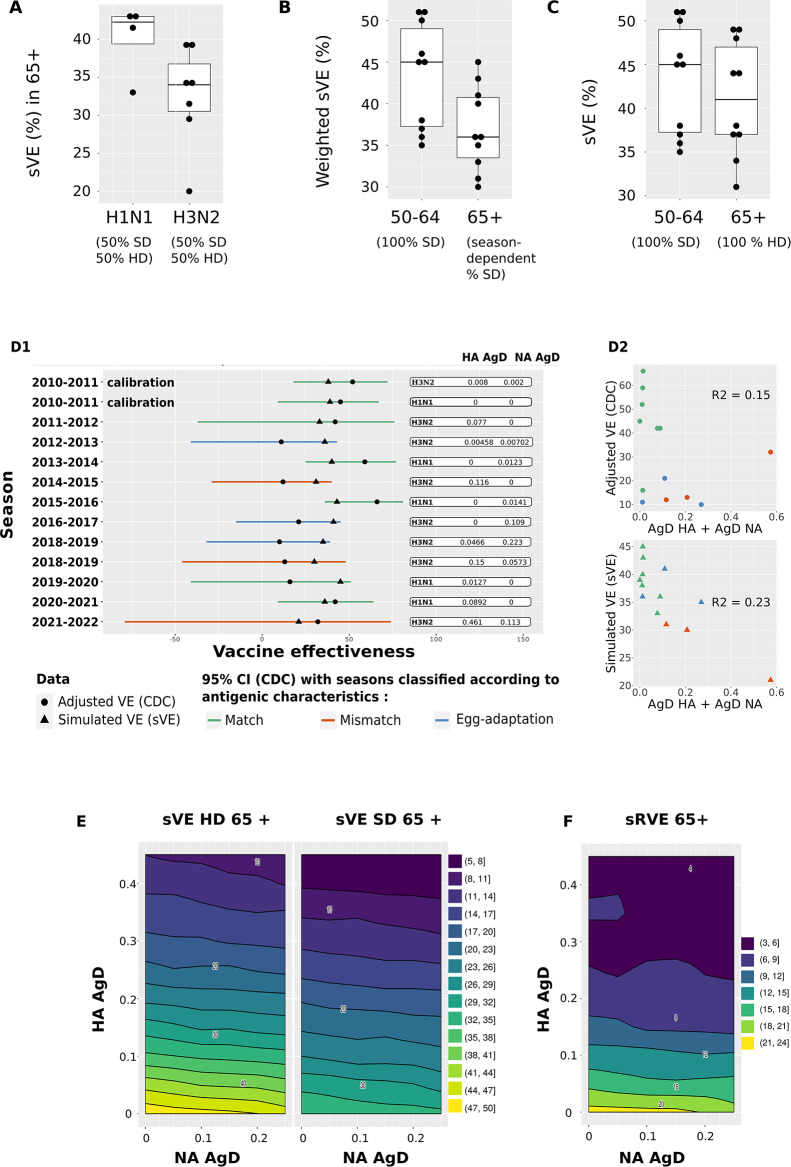
Influenza vaccine effectiveness (VE) varies seasonally due to host, virus and vaccine characteristics. To investigate how antigenic matching and dosage impact VE, we developed a mechanistic knowledge-based mathematical model. Immunization with a split vaccine is modeled for exposure to A/H1N1 or A/H3N2 virus strains. The model accounts for cross-reactivity of immune cells elicited during previous immunizations with new antigens. We simulated vaccine effectiveness (sVE) of high dose (HD) versus standard dose (SD) vaccines in the older population, from 2011 to 2022. We find that sVE is highly dependent on antigenic matching and that higher dosage improves immunogenicity, activation and memory formation of immune cells. In alignment with clinical observations, the HD vaccine performs better than the SD vaccine in all simulations, supporting the use of the HD vaccine in the older population. This model could be adapted to predict the impact of alternative virus strain selection on clinical outcomes in future influenza seasons.
© 2024. The Author(s).
Conflict of interest statement
S.U., M.H., A.I.T., N.R., E.J., E.P., J-B.G., J-P.B., E.C and L. B. are employees of Novadiscovery.S.S.C., L.C. and E.T. are employees of Sanofi and may hold shares and/or stock options in the company. Novadiscovery and Sanofi founded the study.
Figures

References
-
- Centers for disease control and prevention. Disease burden of flu. (2022). https://www.cdc.gov/flu/about/burden/index.html. Accessed: 5th of May 2023.
-
- Smith, D. J. et al. Mapping the antigenic and genetic evolution of influenza virus. Science. 305, 371–376 (2004). - PubMed
-
- Krammer, F. The human antibody response to influenza a virus infection and vaccination. Nat. Rev. Immunol.19(6), 383–397 (2019). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
