

The natural history of neurolymphomatosis
- PMID: 39516680
- PMCID: PMC11523968
- DOI: 10.1038/s44276-024-00053-x
The natural history of neurolymphomatosis
Abstract
Background: Neurolymphomatosis is a lymphoid malignancy of the peripheral nervous system and its natural history is poorly understood.
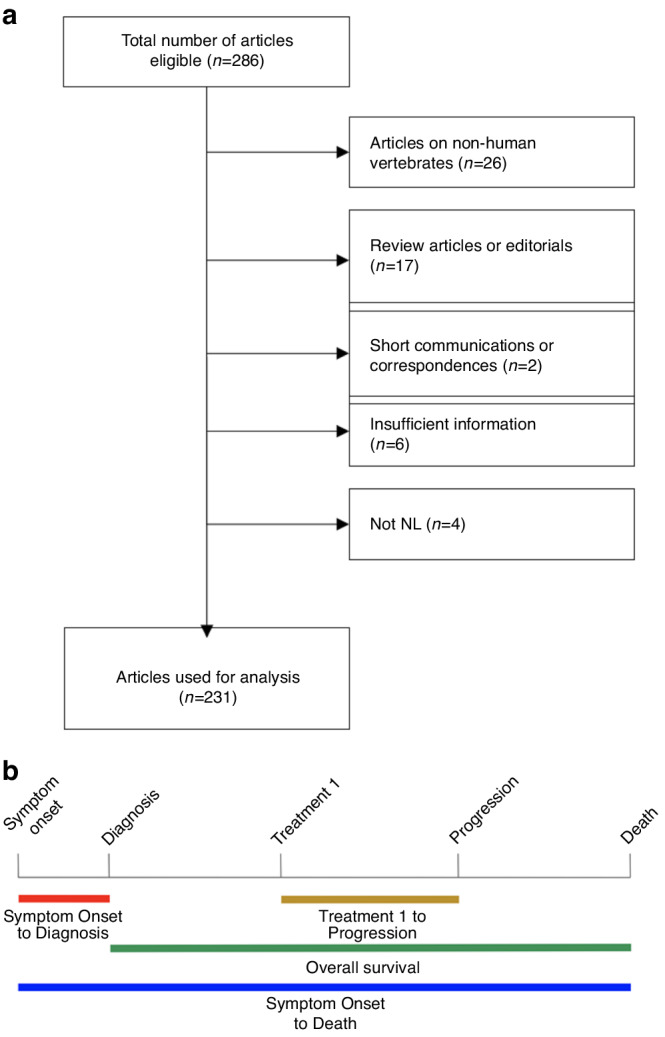
Methods: We performed PubMed search and extracted clinical data for Kaplan-Meier statistics to determine outcome parameters over time. Kruskal-Wallis test was performed to compare prognostic factors.
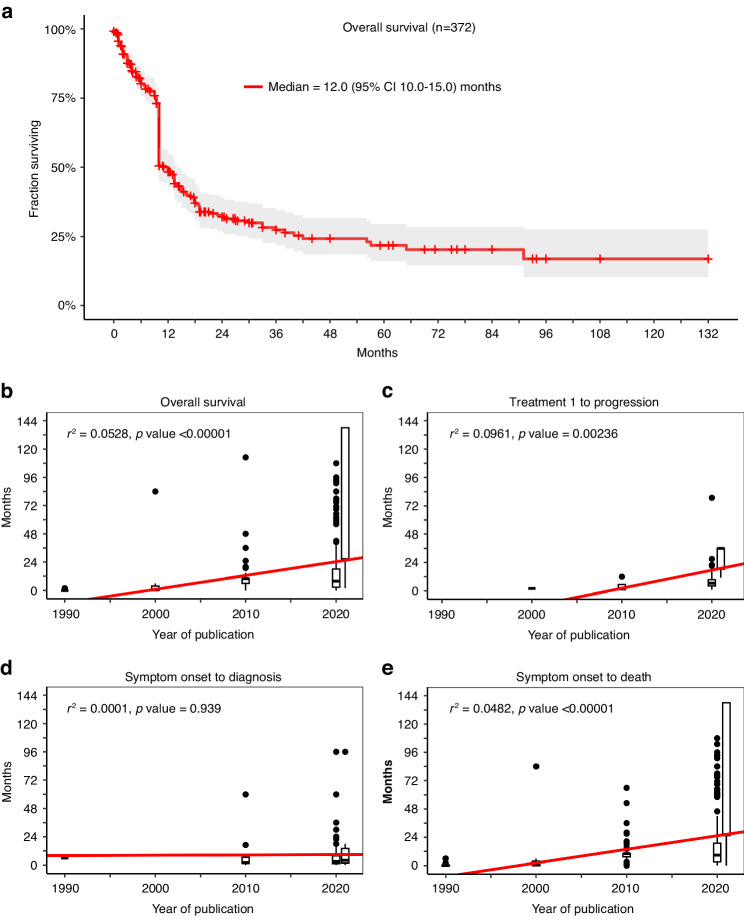
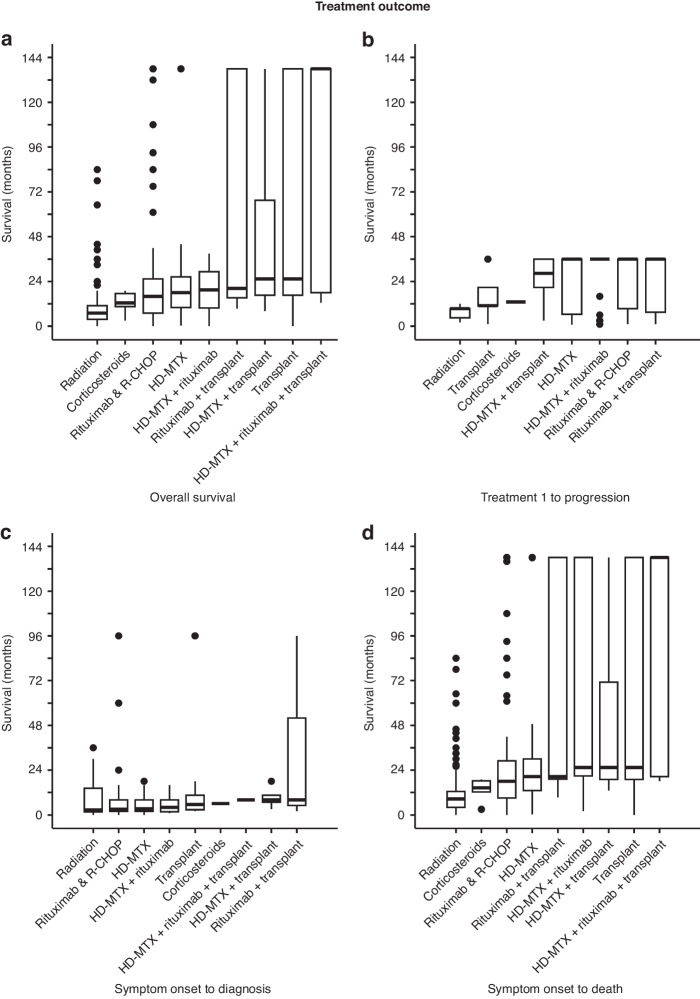
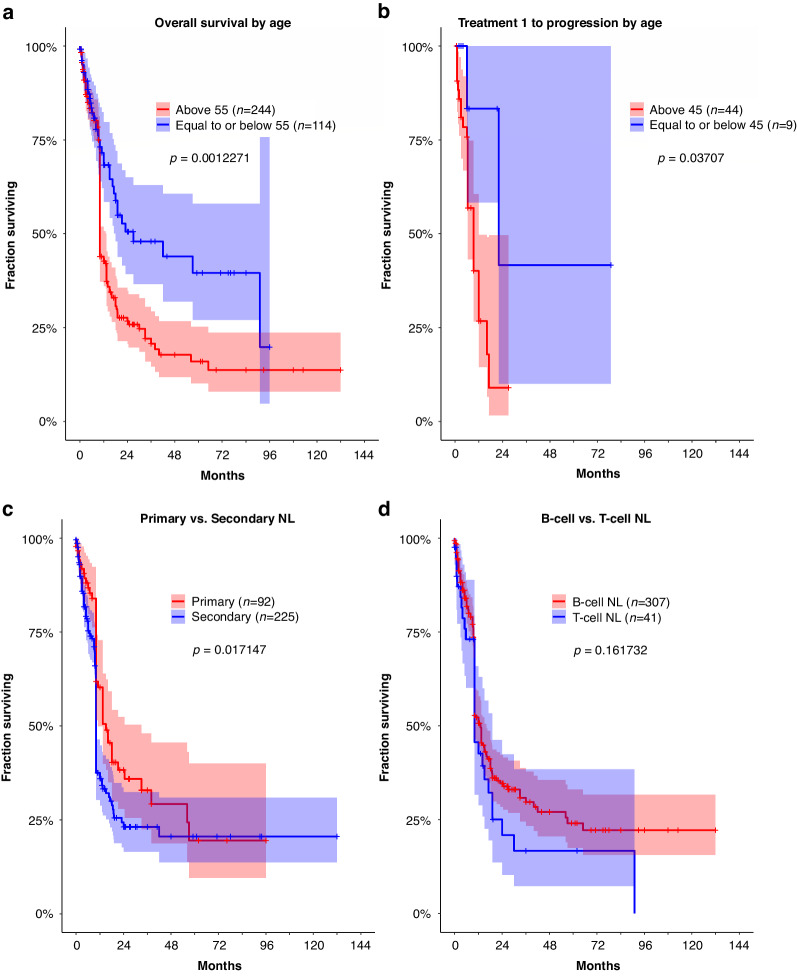
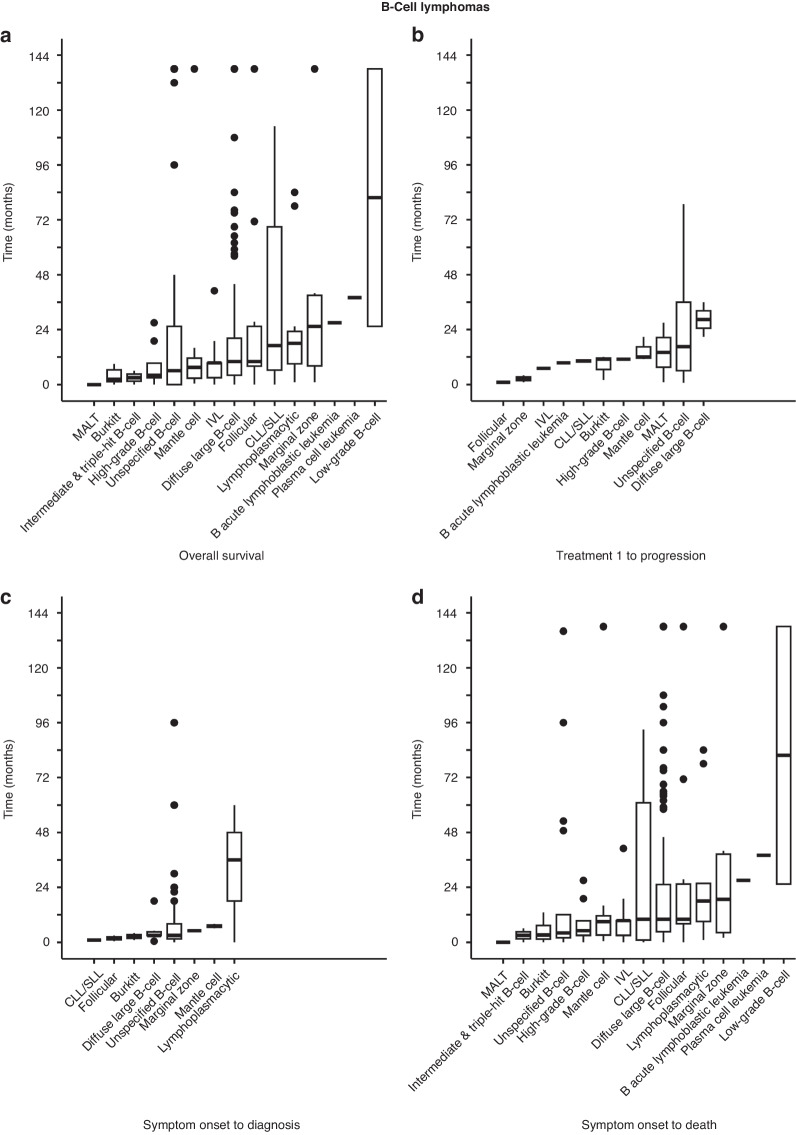
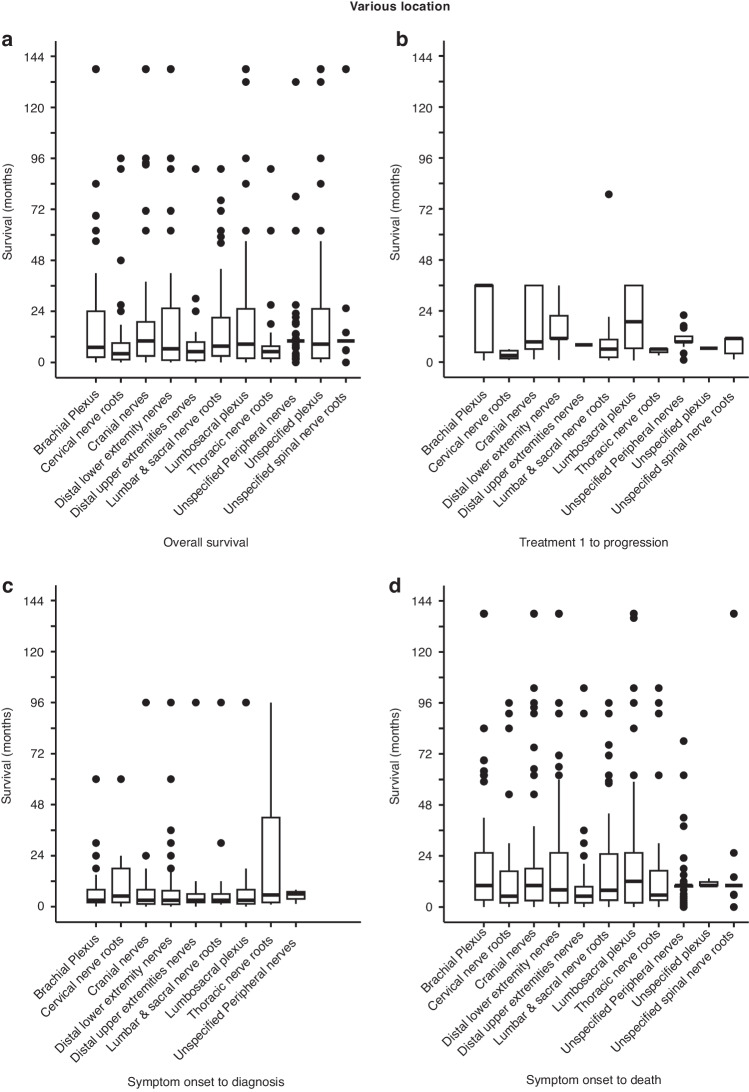
Results: Our search identified 559 patients and their median age was 61 years. Median overall survival (OS) was 12.0 (range 10.0-15.0) months. Diffuse large B-cell lymphoma was the most frequent histology, involving the brachial plexus, cranial nerves, and sciatic nerve. None had molecular profiling. There was a progressive lengthening of OS in successive decades, from 0.5 (95% CI 0.0-0.8) to 26.4 (95% CI 18.0-34.8) months between 1951 and 2022 (r2 = 0.0528, p < 0.00001). Time from first treatment (treatment 1) to progression increased from 2.0 to 36.0 (95% CI 6.5-50.7) months (r2 = 0.0961, p = 0.00236). Time from symptom onset to diagnosis remained unchanged (r2 = 0.0000556, p = 0.939). Patients were most frequently treated with methotrexate, rituximab, and/or radiation either alone or in combination. Primary neurolymphomatosis had a better prognosis than secondary neurolymphomatosis. No OS difference was noted between B- and T-cell disease, but low-grade B-cell performed better than Burkitt's lymphoma.
Discussion: Better outcome for patients with neurolymphomatosis is noted over time. But timely diagnosis remains a major problem that needs improvement.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical Presentation, Management, and Outcome in Neurolymphomatosis: A Systematic Review.Neurology. 2024 Aug 27;103(4):e209698. doi: 10.1212/WNL.0000000000209698. Epub 2024 Aug 5. Neurology. 2024. PMID: 39102613
-
Cranial neurolymphomatosis and its oncologic counterparts: Case series on malignant cranial nerve neuropathies.SAGE Open Med Case Rep. 2023 Dec 30;12:2050313X231221466. doi: 10.1177/2050313X231221466. eCollection 2024. SAGE Open Med Case Rep. 2023. PMID: 38162422 Free PMC article.
-
Primary disease sites and patterns of spread in cases of neurolymphomatosis in the orbit associated with lymphoma.Cancer Imaging. 2021 May 26;21(1):39. doi: 10.1186/s40644-021-00409-3. Cancer Imaging. 2021. PMID: 34039437 Free PMC article.
-
Neurolymphomatosis of the median nerve, optic nerve, L4 spinal nerve root and cauda equina in patients with B-cell malignancies: a case series.J Med Case Rep. 2021 Mar 26;15(1):133. doi: 10.1186/s13256-021-02714-8. J Med Case Rep. 2021. PMID: 33766128 Free PMC article.
-
Primary cauda equina lymphoma confirmed by autopsy: A case report.Neuropathology. 2024 Apr;44(2):147-153. doi: 10.1111/neup.12941. Epub 2023 Aug 28. Neuropathology. 2024. PMID: 37640533 Review.
Cited by
-
Surgical treatment of rare peripheral nerve lesions: long-term outcomes and quality of life.Front Oncol. 2025 Feb 26;14:1476019. doi: 10.3389/fonc.2024.1476019. eCollection 2024. Front Oncol. 2025. PMID: 40078480 Free PMC article.
-
Primary Neurolymphomatosis: A Literature Review.Eur J Neurol. 2025 Apr;32(4):e70173. doi: 10.1111/ene.70173. Eur J Neurol. 2025. PMID: 40265708 Free PMC article. Review.
-
Tafasitamab in refractory diffuse large B-cell lymphoma with neurolymphomatosis.Ann Hematol. 2025 Feb;104(2):1291-1293. doi: 10.1007/s00277-025-06184-6. Epub 2025 Feb 12. Ann Hematol. 2025. PMID: 39934427 Free PMC article.
References
-
- Payne LN, Biggs PM. Studies on Marek’s disease. II. Pathogenesis. J Natl Cancer Inst. 1967;39:281–302. - PubMed
LinkOut - more resources
Full Text Sources