

Timely escalation to second-line therapies after failure of methotrexate in patients with early rheumatoid arthritis does not reduce the risk of becoming difficult-to-treat
- PMID: 39516929
- PMCID: PMC11545058
- DOI: 10.1186/s13075-024-03431-5
Timely escalation to second-line therapies after failure of methotrexate in patients with early rheumatoid arthritis does not reduce the risk of becoming difficult-to-treat
Abstract
Background: To investigate the frequency of difficult-to-treat (D2T) rheumatoid arthritis (RA) in patients early escalated to biologic/targeted synthetic disease modifying anti-rheumatic drugs (b/tsDMARDs) after failure of treat-to-target with methotrexate (MTX).
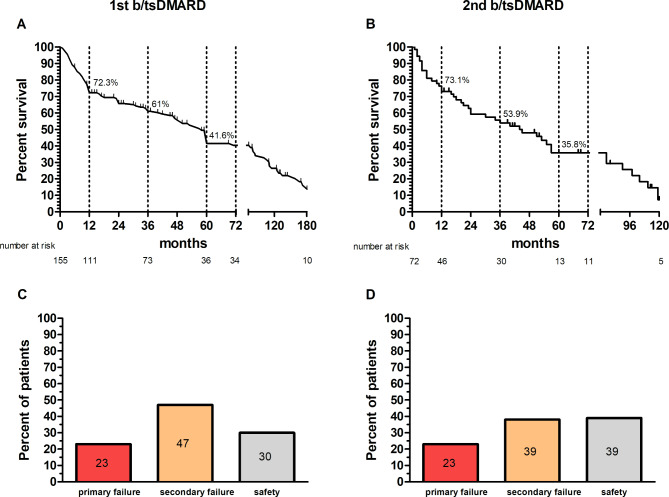
Methods: From a prospective cohort of early RA, all patients with their first access in the years 2005-2018, and eventually starting a b/tsDMARD before the end of 2022, were included and followed-up until April 2024. Study outcomes included drug survival on each consecutive b/tsDMARDs, development of D2T (according to the EULAR definition and subsequent modifications), and its predictors.
Results: Of a total cohort of 722 early RA patients treated with initial MTX and followed-up for at least 3 years from diagnosis, 155 (21.5%) had started a b/tsDMARD after a median of 19 months. In more than 70% of the cases, RA was uncontrolled despite optimal doses of MTX of ≥ 15 mg/day. The retention rates of the first and the second b/tsDMARD were approximatively 70% after 1 year but dropped to 40% after 5 years. After a median (IQR) follow up of 72.6 (34.5-134.2) months, 45 patients (29%) fulfilled the EULAR D2T criteria. At multivariable analysis, higher number of swollen joints and worse pain scores were confirmed as predictors of D2T. Furthermore, in this early RA cohort, shorter disease duration at the start of treatment with b/tsDMARDs, together with negativity for autoantibodies, were also independent predictors of D2T.
Conclusions: Early implementation of treatment after failure of treat-to-target with MTX may not prevent the development of D2T in RA. Patients showing early refractoriness to conventional drugs and those lacking autoantibodies are at higher risk of multiple treatment failures.
Keywords: ACPA; Anti-citrullinated protein antibodies; Difficult-to-treat; Early; Methotrexate; Refractory; Rheumatoid arthritis; Rheumatoid factor; Seronegative; Treat-to-target.
© 2024. The Author(s).
Conflict of interest statement
SB reports grant/research support from: Pfizer, and personal fees from: Alfasigma, AbbVie, Bristol-Myers Squibb, Fresenius Kabi, Lilly, Novartis, UCB. GS reports personal fees from Abbvie, Novartis, Lilly. CM reports personal fees from: Alfasigma, AbbVie, Bristol-Myers Squibb, Lilly, Galapagos, Janssen, Novartis, Pfizer, Sandoz, UCB.
Figures
References
-
- Smolen JS, Landewé RBM, Bergstra SA, Kerschbaumer A, Sepriano A, Aletaha D, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82:3–18. 10.1136/ard-2022-223356. - PubMed
-
- de Hair MJH, Jacobs JWG, Schoneveld JLM, van Laar JM. Difficult-to-treat rheumatoid arthritis: an area of unmet clinical need. Rheumatology (Oxford). 2018;57:1135–44. 10.1093/rheumatology/kex349. - PubMed
-
- Buch MH. Defining refractory rheumatoid arthritis. Ann Rheum Dis. 2018;77:966–9. 10.1136/annrheumdis-2017-212862. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
