

Microbial profile of diabetic foot osteomyelitis from the northwest of England
- PMID: 39516954
- PMCID: PMC11549820
- DOI: 10.1186/s40842-024-00193-6
Microbial profile of diabetic foot osteomyelitis from the northwest of England
Abstract
Background: Osteomyelitis of the diabetic foot is a common and challenging complication affecting patients with diabetic foot ulcers and infections. The complexity of these infections lies in their polymicrobial nature, high rates of persistence and recurrence. This study examined the microbiological profile of diabetic foot osteomyelitis from a teaching hospital in Northwest England and their resistance patterns to understand its impact on infection persistence and to direct effective treatment.
Methods: A retrospective review of 105 patients who underwent surgical management for diabetic foot osteomyelitis between 2019 and 2024. We analysed three consecutive culture samples for each patient to assess for the microbiological profile and resistance patterns of these infections and to monitor infection recurrence and persistence rates.
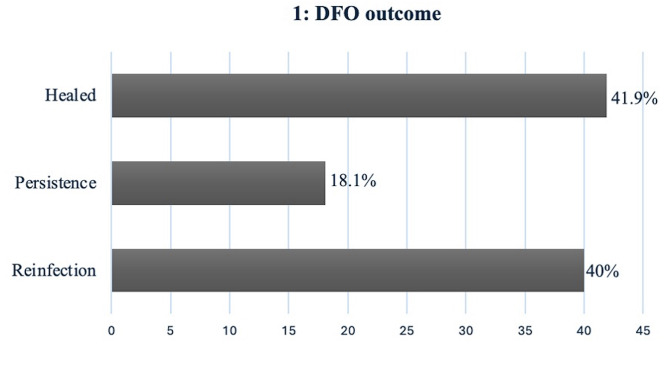
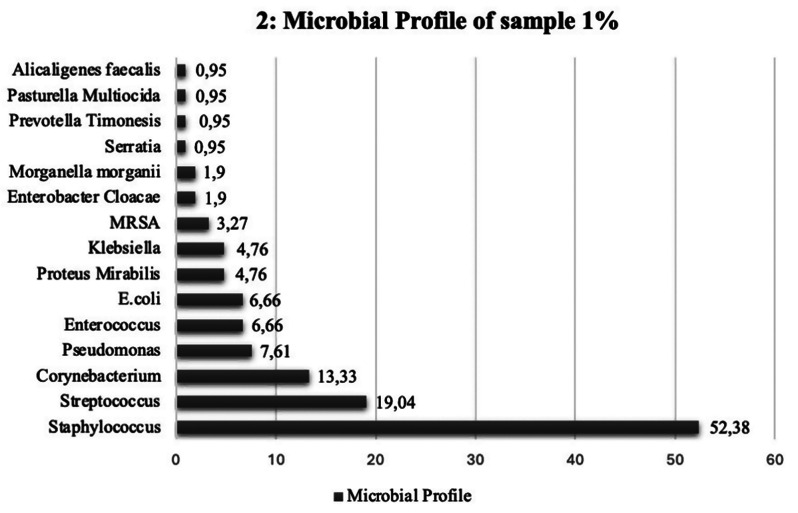
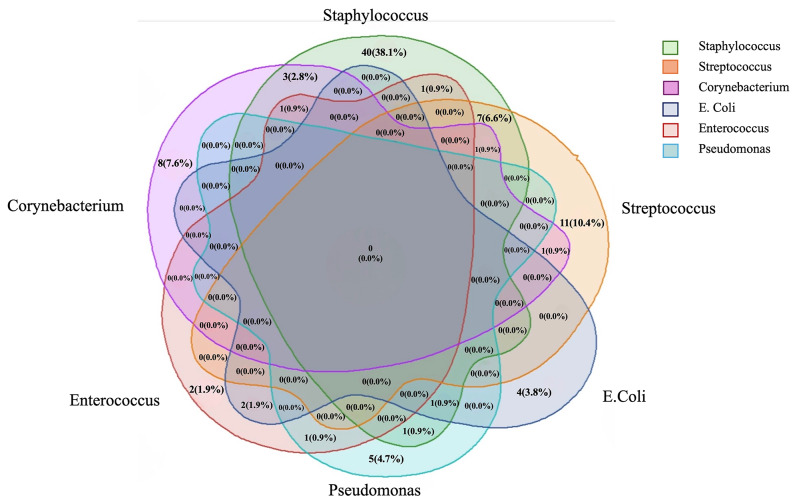
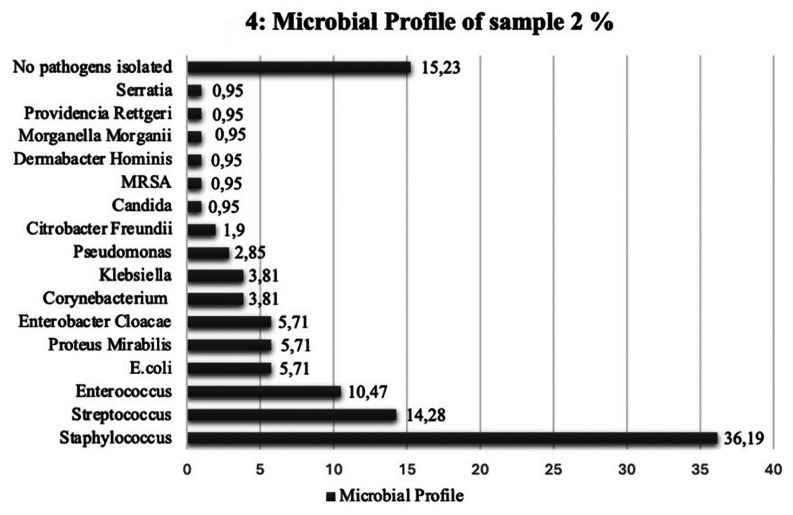
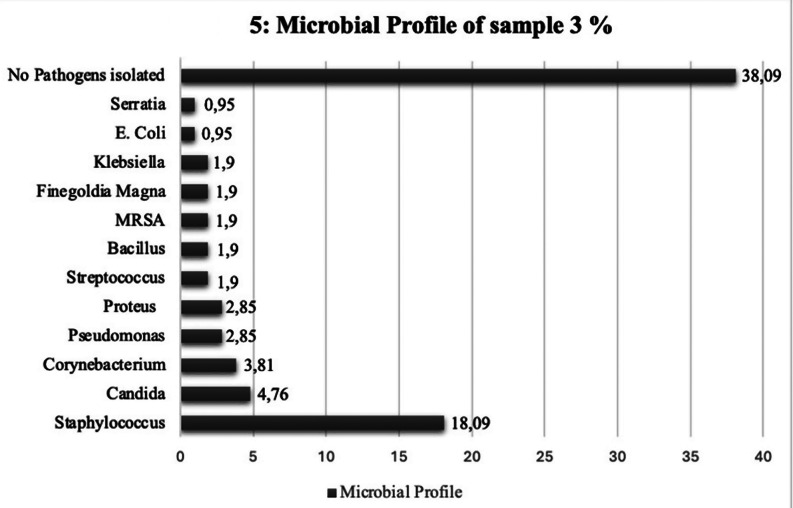
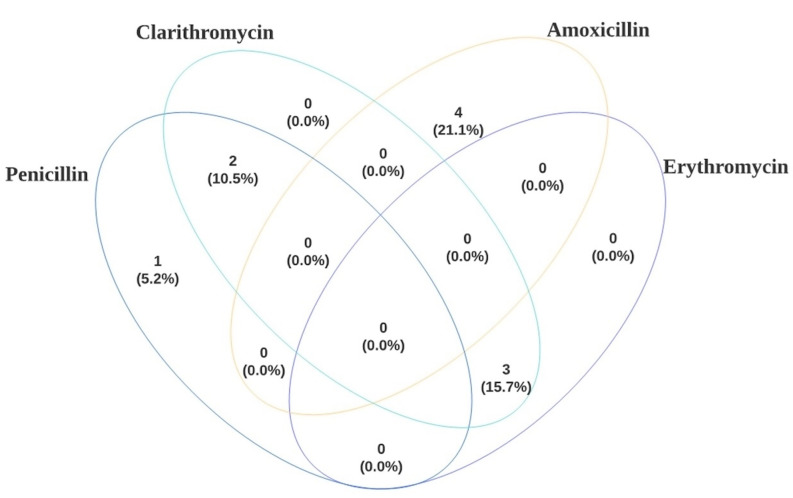
Results: A total of 105 patients were identified. Infection eradication was noted in 42% of the cohort, infection persistence in 18%, and late infection recurrence in 40%. Polymicrobial growth was evident in 72% of our study sample. Gram-positive bacteria made up the majority of the bacterial isolates in all 3 culture samples, 74.81% in sample 1, 69.31% in sample 2, and 55.1% in sample 3. Staphylococcus aureus was the most prevalent gram-positive bacteria, at 52.38% in sample 1, 36.19% in sample 2, and 18.09% in sample 3, followed by Haemolytic Streptococcus, Enterococcus and Corynebacterium. The frequently identified gram-negative bacteria were Pseudomonas in sample 1 (7.61%), E. coli and Proteus in sample 2 (5,71%), Pseudomonas and Proteus in sample 3 (2.85%). Gram-positive bacteria were resistant to penicillin and macrolides with resistance of staphylococcus aureus to clarithromycin identified among all 3 culture samples. Gram-negative bacteria were most resistant to amoxicillin. Staphylococcus aureus was responsible for infection persistence in most of our cohort (12/19) 63.15%. Among those patients, Staphylococcus was resistant to clarithromycin in 6 of the cases. The 5-year mortality rate for our study sample was 32.38%.
Conclusion: This study highlights the prevalence of polymicrobial growth and multi-drug resistant pathogens in the scope of diabetic foot osteomyelitis. It highlights the predominance of Staphylococcus aureus and its resistant strains among patients affected by diabetic foot osteomyelitis in Greater Manchester.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Bacteriological Profile of Diabetic Foot Ulcers and Detection of Methicillin-Resistant Staphylococcus aureus and Extended-Spectrum β-Lactamase Producers in a Tertiary Care Hospital.Cureus. 2021 Dec 22;13(12):e20596. doi: 10.7759/cureus.20596. eCollection 2021 Dec. Cureus. 2021. PMID: 35103172 Free PMC article.
-
Infection Characteristics and Drug Susceptibility of Multidrug-Resistant Bacteria in Patients with Diabetic Foot Ulcers.Clin Lab. 2023 Sep 1;69(9). doi: 10.7754/Clin.Lab.2023.230309. Clin Lab. 2023. PMID: 37702668
-
Identification and antibiotic susceptibility of microorganisms isolated from diabetic foot ulcers: A pathological aspect.Exp Ther Med. 2022 Dec 7;25(1):53. doi: 10.3892/etm.2022.11752. eCollection 2023 Jan. Exp Ther Med. 2022. PMID: 36588808 Free PMC article.
-
Microbial Infection and Antibiotic Susceptibility of Diabetic Foot Ulcer in China: Literature Review.Front Endocrinol (Lausanne). 2022 May 19;13:881659. doi: 10.3389/fendo.2022.881659. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35663325 Free PMC article. Review.
-
Sulopenem: An Intravenous and Oral Penem for the Treatment of Urinary Tract Infections Due to Multidrug-Resistant Bacteria.Drugs. 2022 Apr;82(5):533-557. doi: 10.1007/s40265-022-01688-1. Epub 2022 Mar 16. Drugs. 2022. PMID: 35294769 Review.
Cited by
-
Revisiting Antibiotic-Impregnated Cement Spacer for Diabetic Osteomyelitis of the Foot.Antibiotics (Basel). 2024 Dec 1;13(12):1153. doi: 10.3390/antibiotics13121153. Antibiotics (Basel). 2024. PMID: 39766543 Free PMC article.
References
LinkOut - more resources
Full Text Sources
