

Pituitary hypoadrenocorticism and hypothyroidism after immunochemotherapy followed by salvage surgery for lung cancer: a case report
- PMID: 39516983
- PMCID: PMC11533550
- DOI: 10.1186/s44215-022-00019-w
Pituitary hypoadrenocorticism and hypothyroidism after immunochemotherapy followed by salvage surgery for lung cancer: a case report
Abstract
Background: Immune checkpoint inhibitors (ICIs) have been shown to prolong the survival of patients with non-small cell lung cancer (NSCLC) and have allowed complete resection for advanced lung cancer. However, immune-related adverse events (irAEs) have been recognized as concerning side effects of ICIs.
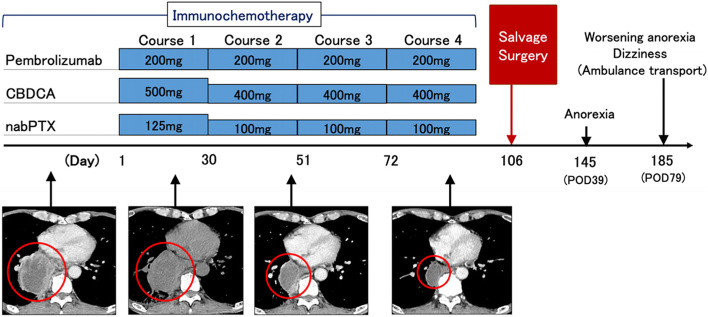
Case presentation: A 62-year-old man visited our hospital because of fever, dyspnea, and anorexia. A tumor was found in the right hilum of the lung. It compressed the left atrium and was also thought to be invading the esophagus and a vertebral body. A bronchoscopic biopsy revealed squamous cell carcinoma of the lung (cT4N2M0-IIIB). We thought that a complete resection was impossible because of the N2 status of the tumor and because it had invaded several organs. Radiotherapy was thought to be contraindicated because of the patient's marked emphysema. Therefore, we administered 4 courses of pembrolizumab plus carboplatin plus nab-paclitaxel immunochemotherapy. After immunochemotherapy, the tumor was downstaged to ycT2bN0M0-IIA and was determined to be acceptable for salvage surgery. A right lower lobectomy and systematic dissection of the mediastinal lymph nodes were performed. The histopathological examination of the resected specimen found that the proportion of the remaining tumor cells was 5%, indicating achievement of a major pathologic response. On postoperative day 79, the patient visited the emergency room because of anorexia. Blood tests showed hyponatremia, hypoglycemia, and eosinophilia. The serum thyroid hormone and thyroid-stimulating hormone levels were low and high, respectively. A corticotropin-releasing hormone stimulation test revealed levels of adrenocorticotropic hormone and cortisol far below the normal ranges. We speculated that the patient had developed pituitary hypoadrenocorticism and hypothyroidism as irAEs associated with ICI treatment. We administered hydrocortisone and levothyroxine, with improvement in the patient's appetite and normalization of the patient's serum sodium level. The patient has been receiving ongoing supplementation with oral hydrocortisone and levothyroxine and is doing well 11 months after surgery.
Conclusions: The increasing numbers of patients treated with perioperative ICIs might lead to increasing numbers of patients who develop perioperative irAEs. Careful attention should be paid to the possible development of irAEs during the perioperative management of patients undergoing surgery for lung cancer.
Keywords: Immune checkpoint inhibitor; Immune-related adverse events; Immunochemotherapy; Lung cancer; Surgery.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
[Pituitary immune-related adverse events induced by programmed cell death protein 1 inhibitors in advanced lung cancer patients: A report of 3 cases].Beijing Da Xue Xue Bao Yi Xue Ban. 2022 Apr 18;54(2):369-375. doi: 10.19723/j.issn.1671-167X.2022.02.027. Beijing Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35435206 Free PMC article. Chinese.
-
Pembrolizumab-Induced Hypophysitis: A Rare Immune-Related Adverse Event in a Patient With Metastatic Non-small Cell Lung Cancer.Cureus. 2025 Apr 21;17(4):e82701. doi: 10.7759/cureus.82701. eCollection 2025 Apr. Cureus. 2025. PMID: 40400852 Free PMC article.
-
Hypothyroidism and hypopituitarism as immune-related adverse events due to lenvatinib plus pembrolizumab therapy in the immediate postoperative period after laparoscopic hepatectomy for liver metastases from gastric cancer: a case report.Surg Case Rep. 2021 Dec 20;7(1):267. doi: 10.1186/s40792-021-01346-w. Surg Case Rep. 2021. PMID: 34928436 Free PMC article.
-
Isolated adrenocorticotropic hormone deficiency associated with sintilimab therapy in a patient with advanced lung adenocarcinoma: a case report and literature review.BMC Endocr Disord. 2022 Sep 24;22(1):239. doi: 10.1186/s12902-022-01151-y. BMC Endocr Disord. 2022. PMID: 36153581 Free PMC article. Review.
-
Isolated adrenocorticotropic hormone deficiency and thyroiditis associated with nivolumab therapy in a patient with advanced lung adenocarcinoma: a case report and review of the literature.J Med Case Rep. 2019 Mar 26;13(1):88. doi: 10.1186/s13256-019-2002-2. J Med Case Rep. 2019. PMID: 30909965 Free PMC article. Review.
Cited by
-
Real-world safety of carboplatin in non-small cell lung cancer: a retrospective signal detection and subgroup analysis based on the FAERS database.Front Med (Lausanne). 2025 Jun 16;12:1590738. doi: 10.3389/fmed.2025.1590738. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40589971 Free PMC article.
References
-
- Yamaguchi M, Nakagawa K, Suzuki K, Takamochi K, Ito H, Okami J, et al. Surgical challenges in multimodal treatment of N2-stage IIIA non-small cell lung cancer. Jpn J Clin Oncol. 2021;51:333–44. - PubMed
-
- Provencio M, Nadal E, Insa A, García-Campelo MR, Casal-Rubio J, Dómine M, et al. Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell lung cancer (NADIM): an open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020;21:1413–22. - PubMed
LinkOut - more resources
Full Text Sources