

The Neurological and Hemodynamics Safety of an Airway Clearance Technique in Patients with Acute Brain Injury: An Analysis of Intracranial Pressure Pulse Morphology Using a Non-Invasive Sensor
- PMID: 39517963
- PMCID: PMC11548518
- DOI: 10.3390/s24217066
The Neurological and Hemodynamics Safety of an Airway Clearance Technique in Patients with Acute Brain Injury: An Analysis of Intracranial Pressure Pulse Morphology Using a Non-Invasive Sensor
Abstract
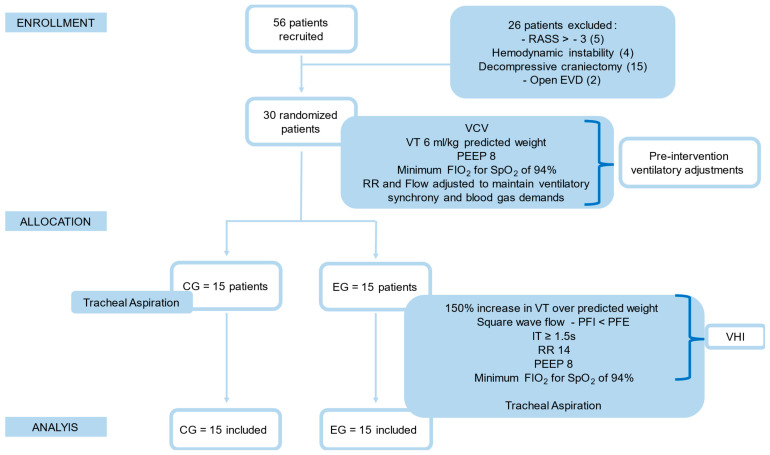
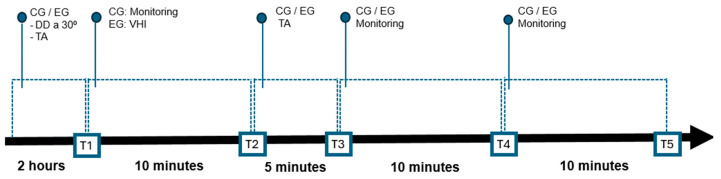
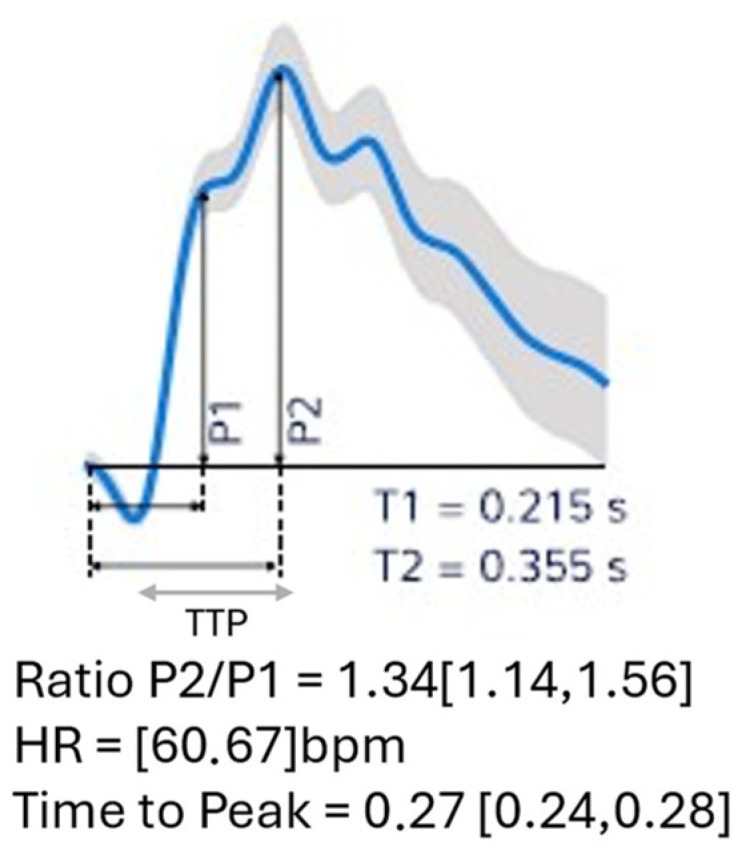
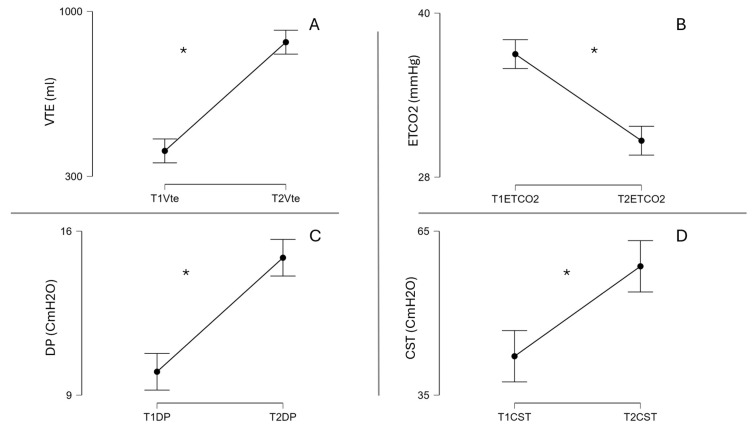
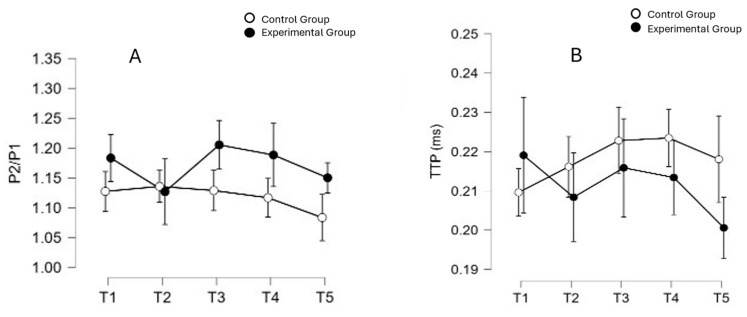
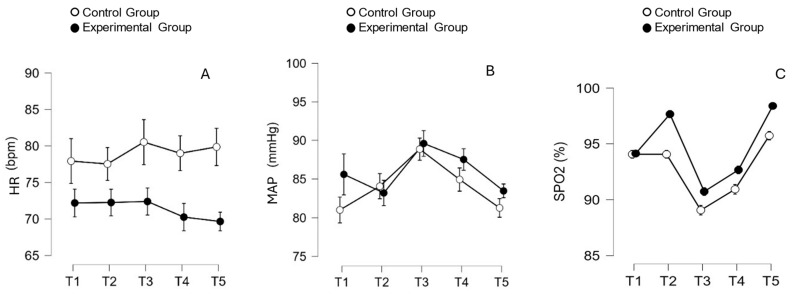
Patients with acute brain injury (ACI) often require mechanical ventilation (MV) and are subject to pulmonary complications, thus justifying the use of Airway Clearance Techniques (ACTs), but their effects on intracranial pressure (ICP) are unknown. This study investigates the neurological and hemodynamics safety of an ACT called ventilator hyperinflation (VHI) in patients with ACI. This was a randomized clinical equivalence trial, which included patients aged ≥ 18 years with a clinical diagnosis of hemorrhagic stroke, with symptom onset within 48 h. The participants were randomly allocated to the Experimental Group (EG, n = 15), which underwent VHI followed by tracheal aspiration (TA), and the Control Group (CG, n = 15), which underwent TA only. Neurological safety was verified by analyzing the morphology of the ICP wave through the non-invasive B4C sensor, which detects bone deformation of the skull, resulting in a P2/P1 ratio and TTP, and hemodynamics through a multi-parameter monitor. Evaluations were recorded during five instances: T1 (baseline/pre-VHI), T2 (post-VHI and before TA), T3 (post-TA), T4 and T5 (monitoring 10 and 20 min after T3). The comparison between groups showed that there was no effect of the technique on the neurological variables with a mean P2/P1 ratio [F (4,112) = 1.871; p = 0.120; np2 = 0.063] and TTP [F (4,112) = 2.252; p = 0.068; np2 = 0.074], and for hemodynamics, heart rate [F (4,112) = 1.920; p = 0.112; np2 = 0.064] and mean arterial pressure [F(2.73, 76.57) = 0.799; p = 0.488; np2 = 0.028]. Our results showed that VHI did not pose a neurological or hemodynamics risk in neurocritical patients after ACI.
Keywords: ICP wave morphology; intracranial compliance; intracranial pressure; mechanical ventilation; mucociliary clearance; non-invasive intracranial pressure monitor; ventilator hyperinflation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Beqiri E., Smielewski P., Guérin C., Czosnyka M., Robba C., Bjertnæs L., Frisvold S.K. Neurological and respiratory effects of lung protective ventilation in acute brain injury patients without lung injury: Brain vent, a single centre randomized interventional study. Crit. Care. 2023;27:115. doi: 10.1186/s13054-023-04383-z. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
