

Developmental Patterns and Risk Factors of Scoliosis After Hemipelvectomy for the Pelvic Bone Tumor
- PMID: 39518360
- PMCID: PMC11545142
- DOI: 10.3390/diagnostics14212392
Developmental Patterns and Risk Factors of Scoliosis After Hemipelvectomy for the Pelvic Bone Tumor
Abstract
Background: Postoperative scoliosis is often seen after hemipelvectomy for malignancies involving the pelvic area, but the details remain unclear. The objectives were to investigate the development patterns and risk factors of scoliosis after hemipelvectomy.
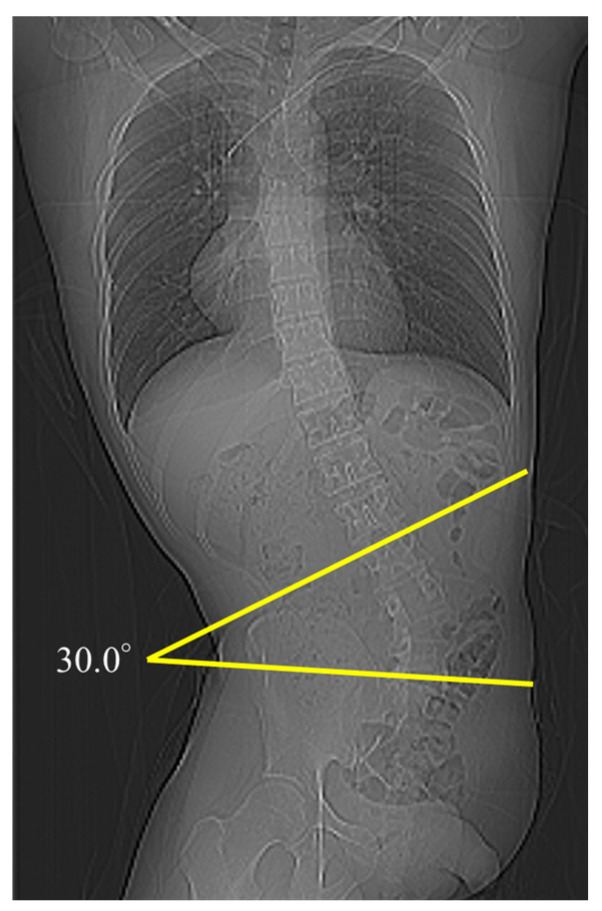
Methods: We retrospectively reviewed 30 patients who underwent hemipelvectomy at our hospital between 1998 and 2020. The risk factors of scoliosis with a Cobb angle of ≥10° were investigated.
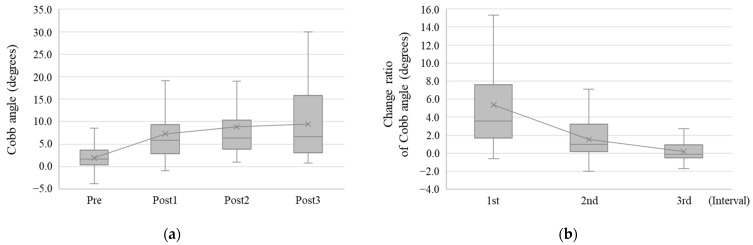
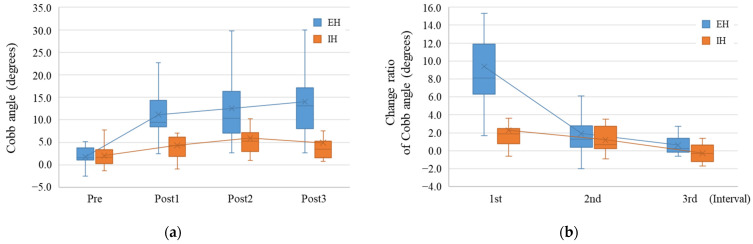
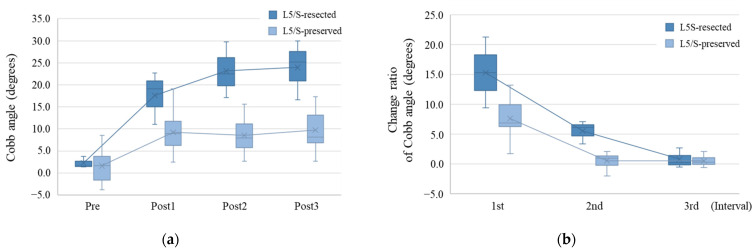
Results: The postoperative Cobb angle significantly increased in all patients compared with the preoperative one (p < 0.001), and the change ratio of the Cobb angle was significantly higher during the first postoperative year than thereafter. The external hemipelvectomy (EH) group demonstrated a larger Cobb angle and a higher change ratio than the internal hemipelvectomy group. Nine patients developed scoliosis with a final Cobb angle of ≥10°, and the risk factors were EH (p = 0.017), P1+2+3+4 resection according to the Enneking classification (p = 0.005), iliac crest resection (p = 0.004), L5/S resection (p = 0.020), and no pelvic ring reconstruction after hemipelvectomy (p = 0.004).
Conclusions: Approximately 30% of patients who underwent hemipelvectomy developed scoliosis with a Cobb angle of ≥10°, and this angle increased rapidly during the first postoperative year. Hence, careful follow-up of scoliosis is required after hemipelvectomy.
Keywords: hemipelvectomy; sarcoma; scoliosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Pelvic ring reconstruction with a double-barreled free vascularized fibula graft after resection of malignant pelvic bone tumor.Arch Orthop Trauma Surg. 2015 May;135(5):619-25. doi: 10.1007/s00402-015-2197-7. Epub 2015 Mar 21. Arch Orthop Trauma Surg. 2015. PMID: 25795428 Free PMC article.
-
Does adding sacroiliac (type IV) resection to periacetabular (type II) resection increase complications or provide worse clinical outcomes? An institutional experience and systematic review.Surg Oncol. 2024 Oct;56:102116. doi: 10.1016/j.suronc.2024.102116. Epub 2024 Aug 8. Surg Oncol. 2024. PMID: 39128439
-
Analysis of the factors affecting the loss of correction effect in patients with congenital scoliosis after one stage posterior hemivertebrae resection and orthosis fusion.BMC Musculoskelet Disord. 2023 Dec 11;24(1):960. doi: 10.1186/s12891-023-07060-y. BMC Musculoskelet Disord. 2023. PMID: 38082325 Free PMC article.
-
External and internal hemipelvectomy: A retrospective analysis of 68 cases.Jt Dis Relat Surg. 2022;33(1):132-141. doi: 10.52312/jdrs.2022.560. Epub 2022 Mar 28. Jt Dis Relat Surg. 2022. PMID: 35361087 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
References
-
- Guder W.K., Hardes J., Gosheger G., Henrichs M.P., Nottrott M., Streitburger A. Analysis of surgical and oncological outcome in internal and external hemipelvectomy in 34 patients above the age of 65 years at a mean follow-up of 56 months. BMC Musculoskelet. Disord. 2015;16:33. doi: 10.1186/s12891-015-0494-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
