

Osteoporosis and Normocalcemic Primary Hyperparathyroidism (Conservatively or Surgically Managed)
- PMID: 39518465
- PMCID: PMC11545940
- DOI: 10.3390/jcm13216325
Osteoporosis and Normocalcemic Primary Hyperparathyroidism (Conservatively or Surgically Managed)
Abstract
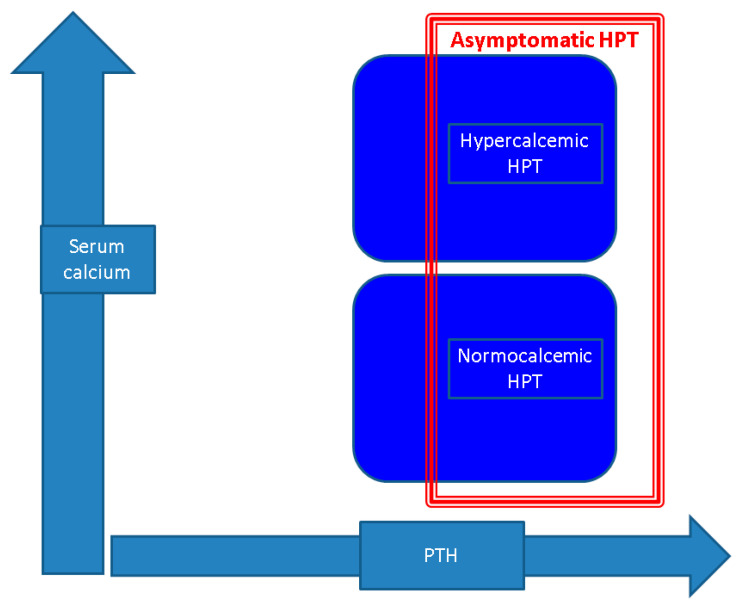
Asymptomatic primary hyperparathyroidism (PHPT) involves 80-90% of the parathyroid tumor-associated cases of PHPT in the modern medical era, while normocalcemic PHPT (NPHPT) has a prevalence of 0.1-11%. We aimed to analyze the bone status and mineral metabolism in NPHPT amid conservative or surgical management. In this narrative review, we searched PubMed (between January 2020 and July 2024) via different keywords. Fourteen studies from the final analysis (388 patients with NPHPT; 1188 with PHPT; and 803 controls) showed that mean serum calcium levels varied between 2.57 and 2.26 mmol/L in NPHPT. Ten studies identified a similar 24 h urinary calcium in NPHPT versus hypercalcemic PHPT (HPHPT). Except for one study, a mandatory vitamin D analysis was performed, but the 25-hydroxyvitamin D cut-offs varied. Osteoporosis (n = 6 studies; N = 172 with NPHPT) was confirmed in 41.7-100% of NPHPT subjects. In surgery candidates, this rate might be overestimated. A DXA analysis was performed in eight studies (235 subjects with NPHPT, and 455 patients with HPHPT); two studies identified a lower BMD in HPHPT < NPHPT, but the results were not homogenous. A single study analyzed the TBS and found similar results in NPHPT. The prevalence of fractures (n = 9) varied between 7.4% and 42.8% in NPHPT. Bone turnover markers (N = 262 patients, n = 8 studies) showed lower bone formation markers in NPHPT versus PHPT (n = 3). Two studies analyzed the BMD and bone turnover markers following parathyroidectomy (161 patients, including 30 patients with NPHPT; mean ages over 60 years). To conclude, given the wide spectrum of complications associated with PHPT, an early diagnosis and proper management is essential. A more extensive screening in patients with osteoporosis and kidney stones might lead to the discovery of NPHPT, a more recently described form of PHPT. While it is still unclear whether NPHPT is an early stage of HPHPT or a separate entity, recent findings show similar osteoporosis and fracture occurrence, and an improvement in bone metabolism, following parathyroidectomy. More extensive prospective studies are crucial to understand the natural course of the disease, to reach a consensus regarding parathyroidectomy indications and surgery candidates' selection, and to ensure proper personalized management for these patients. With the evolving diagnosis methods, PHPT has become a condition with a changing clinical presentation, which now requires modern evaluation and treatment approaches.
Keywords: DXA; PTH; TBS; calcium; fracture; metabolism; parathyroid tumor; parathyroidectomy; surgery; vitamin D.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
