Chest Tubes and Pleural Drainage: History and Current Status in Pleural Disease Management
- PMID: 39518470
- PMCID: PMC11547156
- DOI: 10.3390/jcm13216331
Chest Tubes and Pleural Drainage: History and Current Status in Pleural Disease Management
Abstract
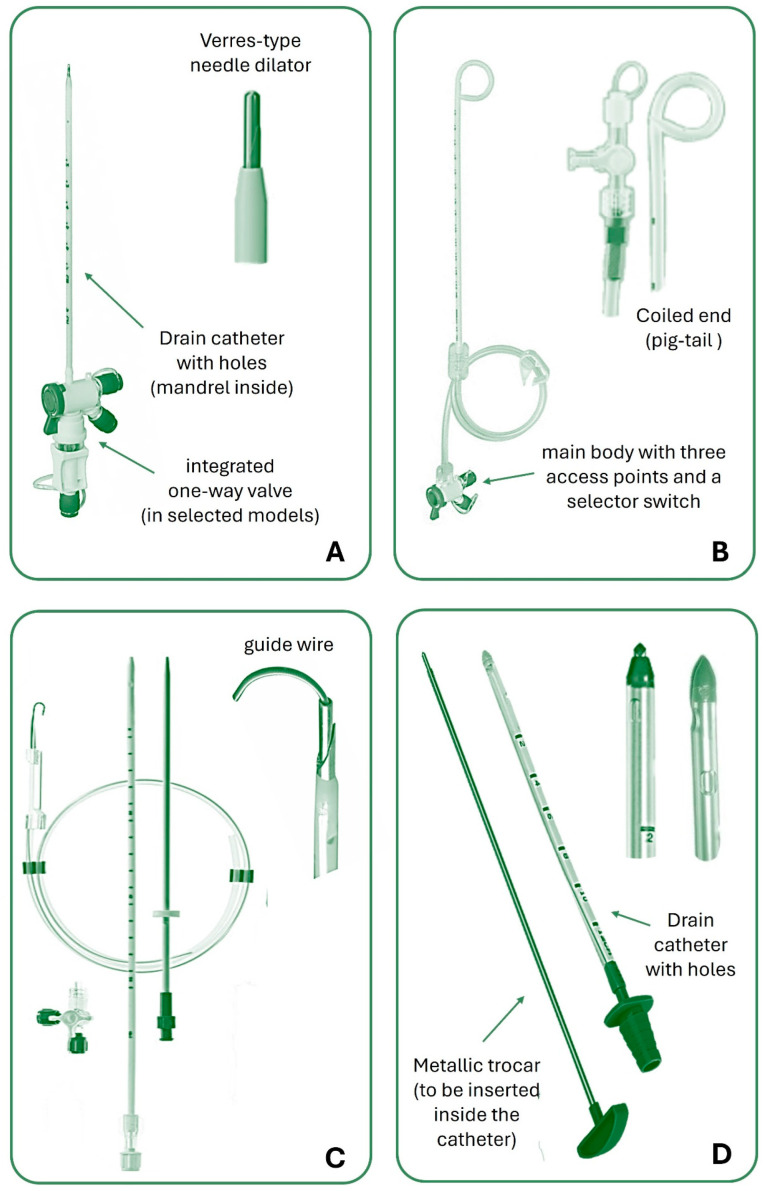
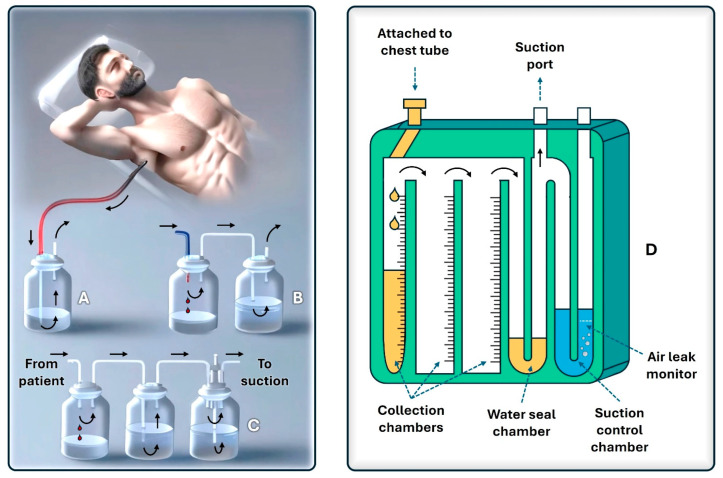
Thoracostomy and chest tube placement are key procedures in treating pleural diseases involving the accumulation of fluids (e.g., malignant effusions, serous fluid, pus, or blood) or air (pneumothorax) in the pleural cavity. Initially described by Hippocrates and refined through the centuries, chest drainage achieved a historical milestone in the 19th century with the creation of closed drainage systems to prevent the entry of air into the pleural space and reduce infection risk. The introduction of plastic materials and the Heimlich valve further revolutionized chest tube design and function. Technological advancements led to the availability of various chest tube designs (straight, angled, and pig-tail) and drainage systems, including PVC and silicone tubes with radiopaque stripes for better radiological visualization. Modern chest drainage units can incorporate smart digital systems that monitor and graphically report pleural pressure and evacuated fluid/air, improving patient outcomes. Suction application via wall systems or portable digital devices enhances drainage efficacy, although careful regulation is needed to avoid complications such as re-expansion pulmonary edema or prolonged air leak. To prevent recurrent effusion, particularly due to malignancy, pleurodesis agents can be applied through the chest tube. In cases of non-expandable lung, maintaining a long-term chest drain may be the most appropriate approach and procedures such as the placement of an indwelling pleural catheter can significantly improve quality of life. Continued innovations and rigorous training ensure that chest tube insertion remains a cornerstone of effective pleural disease management. This review provides a comprehensive overview of the historical evolution and modern advancements in pleural drainage. By addressing both current technologies and procedural outcomes, it serves as a valuable resource for healthcare professionals aiming to optimize pleural disease management and patient care.
Keywords: chest tube; drainage; empyema; pleural effusion; pneumothorax.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures