

Finerenone: A Third-Generation MRA and Its Impact on Cardiovascular Health-Insights from Randomized Controlled Trials
- PMID: 39518537
- PMCID: PMC11547165
- DOI: 10.3390/jcm13216398
Finerenone: A Third-Generation MRA and Its Impact on Cardiovascular Health-Insights from Randomized Controlled Trials
Abstract
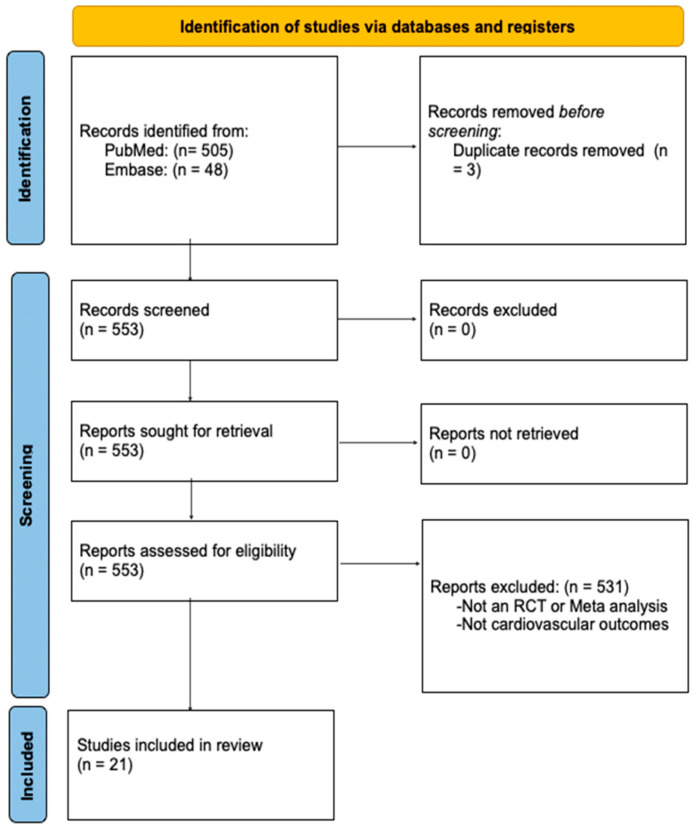
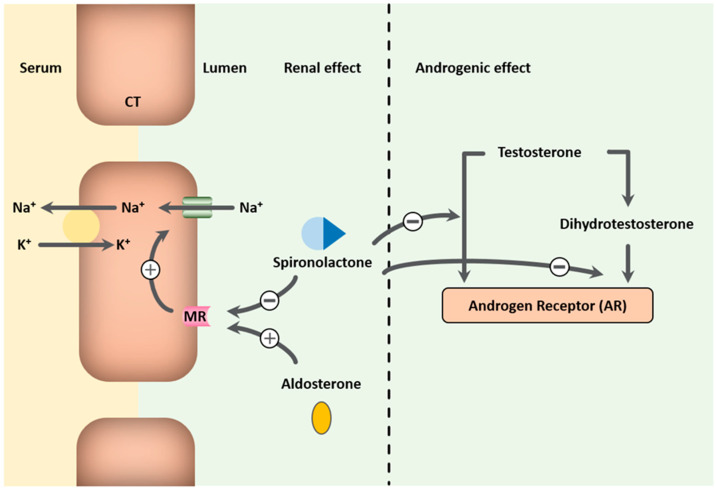
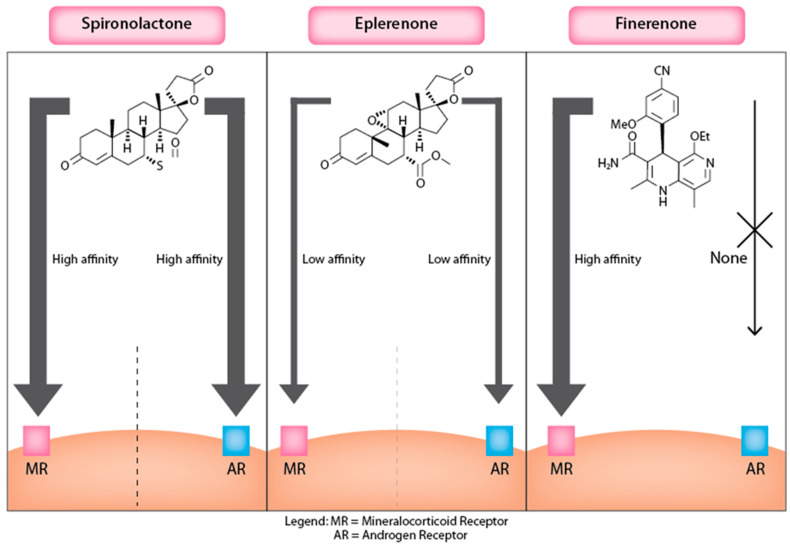
Introduction: Finerenone, a third-generation non-steroidal mineralocorticoid receptor antagonist (MRA), offers a targeted approach to managing cardiovascular outcomes, particularly in patients with chronic kidney disease (CKD) and type 2 diabetes (T2D). Unlike traditional MRAs such as spironolactone and eplerenone, which can cause off-target hormonal side effects and hyperkalemia, Finerenone selectively binds to mineralocorticoid receptors, reducing these risks. Recent randomized controlled trials have demonstrated Finerenone's potential to improve cardiovascular outcomes, making it a promising alternative in the management of heart failure and other cardiovascular conditions associated with CKD and T2D. Methods: We conducted a scoping review using PRISMA guidelines. A search for "Finerenone" in the PubMed, Embase, and Cochrane Library databases included randomized controlled trials (RCTs), post hoc analyses, and relevant meta-analyses on cardiovascular outcomes. Data were synthesized narratively, assessing study quality through strengths and limitations. Discussion: Finerenone has shown significant benefits and a superior safety profile compared with traditional MRAs like spironolactone and eplerenone in managing CKD, T2D, and heart failure. It effectively reduces cardiovascular and renal events while minimizing risks such as hyperkalemia and hormonal side effects associated with steroidal MRAs. Future studies, including the REDEFINE-HF, FINALITY-HF, and CONFIRMATION-HF trials, will further explore Finerenone's potential across diverse heart failure phenotypes, including its role in heart failure with mildly reduced and preserved ejection fractions, potentially establishing it as a cornerstone therapy in heart failure management. Conclusions: Finerenone represents a significant advancement in MRA therapy, offering enhanced safety and efficacy in managing cardiovascular outcomes in CKD and T2D patients. The current evidence supports its use as a promising alternative to traditional MRAs, particularly in patients intolerant to steroidal MRAs. Further trials are needed to fully establish its potential across diverse patient populations, including those with varying heart failure phenotypes.
Keywords: eplerenone; finerenone; heart failure; spironolactone; steroidal mineralocorticoid receptor antagonist; systematic review.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Effectiveness of nonsteroidal mineralocorticoid receptor antagonists in patients with diabetic kidney disease.Postgrad Med. 2023 Apr;135(3):224-233. doi: 10.1080/00325481.2022.2060598. Epub 2022 Apr 20. Postgrad Med. 2023. PMID: 35392754 Review.
-
Pharmacology and Therapeutic Potential of Finerenone: A Novel Third-Generation Nonsteroidal Mineralocorticoid Receptor Antagonist.Cureus. 2025 Jul 11;17(7):e87706. doi: 10.7759/cureus.87706. eCollection 2025 Jul. Cureus. 2025. PMID: 40786373 Free PMC article. Review.
-
Finerenone's Impact on Major Adverse Cardiovascular Events in Chronic Kidney Disease and Type 2 Diabetes Mellitus: A Systematic Review.Cureus. 2024 Aug 31;16(8):e68274. doi: 10.7759/cureus.68274. eCollection 2024 Aug. Cureus. 2024. PMID: 39350809 Free PMC article. Review.
-
Finerenone: a breakthrough mineralocorticoid receptor antagonist for heart failure, diabetes and chronic kidney disease.Egypt Heart J. 2024 Dec 16;76(1):159. doi: 10.1186/s43044-024-00586-z. Egypt Heart J. 2024. PMID: 39680348 Free PMC article. Review.
-
A comprehensive review of finerenone-a third-generation non-steroidal mineralocorticoid receptor antagonist.Front Cardiovasc Med. 2024 Sep 23;11:1476029. doi: 10.3389/fcvm.2024.1476029. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39376623 Free PMC article. Review.
Cited by
-
Now and the Future: Medications Changing the Landscape of Cardiovascular Disease and Heart Failure Management.J Clin Med. 2025 Jun 3;14(11):3948. doi: 10.3390/jcm14113948. J Clin Med. 2025. PMID: 40507711 Free PMC article. Review.
References
-
- Yancy C.W., Jessup M., Bozkurt B., Butler J., Casey D.E., Jr., Colvin M.M., Drazner M.H., Filippatos G.S., Fonarow G.C., Givertz M.M., et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll. Cardiol. 2017;70:776–803. - PubMed
-
- McMurray J.J., Adamopoulos S., Anker S.D., Auricchio A., Böhm M., Dickstein K., Falk V., Filippatos G., Fonseca C., Gomez-Sanchez M.A., et al. ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012;33:1787–1847. doi: 10.1093/eurheartj/ehs104. - DOI - PubMed
-
- Young D.B., Smith M.J., Jr., Jackson T.E., Scott R.E. Multiplicative interaction between angiotensin II and K concentration in stim-ulation of aldosterone. Am. J. Physiol. 1984;247:E328. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
