

Hip Flexor Muscle Activation During Common Rehabilitation and Strength Exercises
- PMID: 39518756
- PMCID: PMC11546833
- DOI: 10.3390/jcm13216617
Hip Flexor Muscle Activation During Common Rehabilitation and Strength Exercises
Abstract
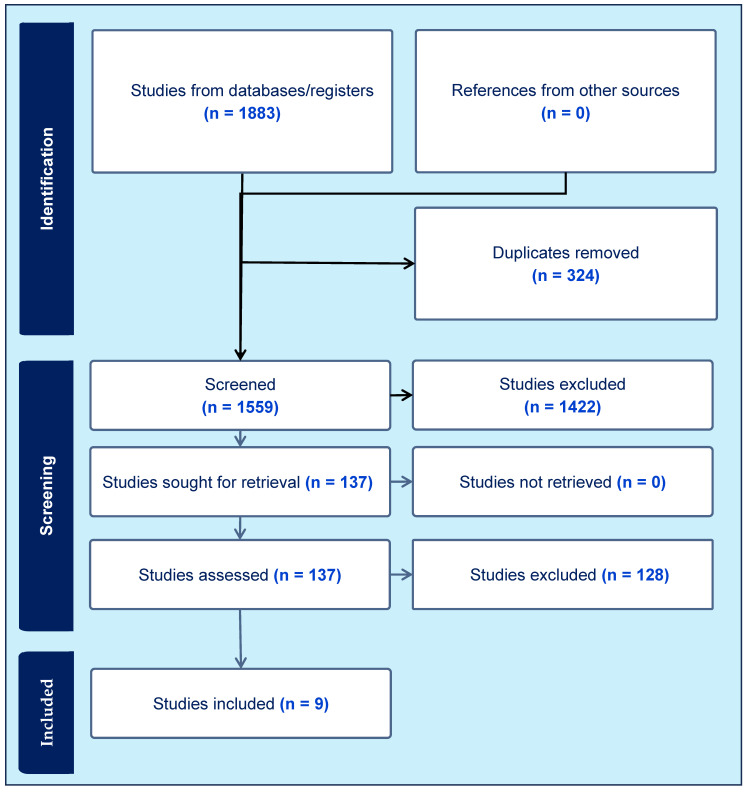
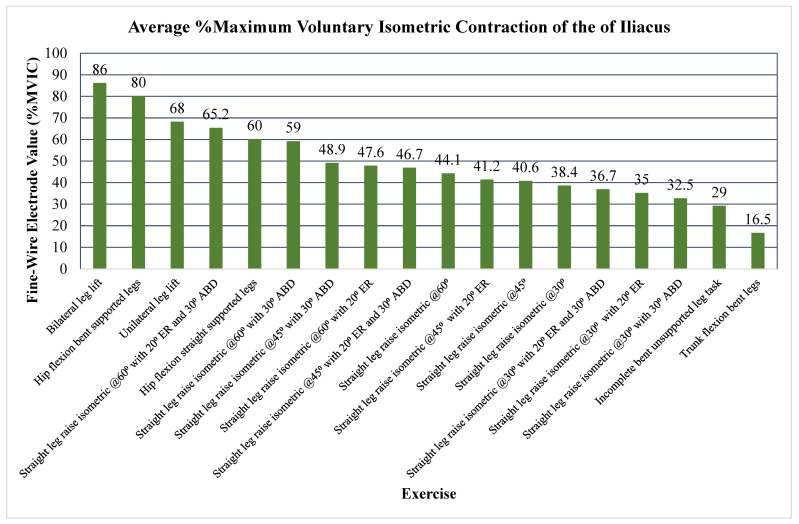
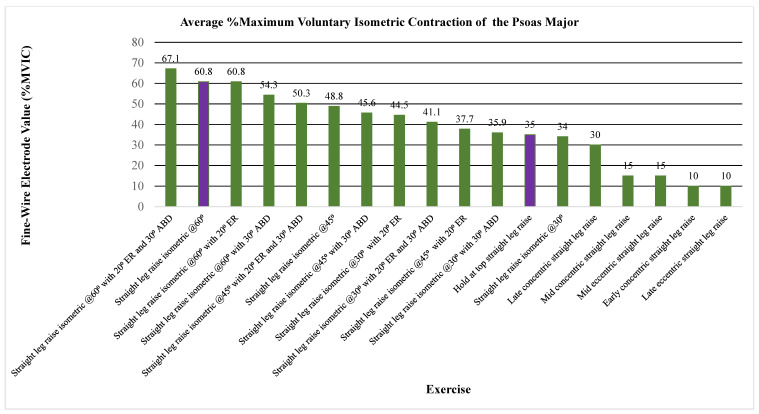
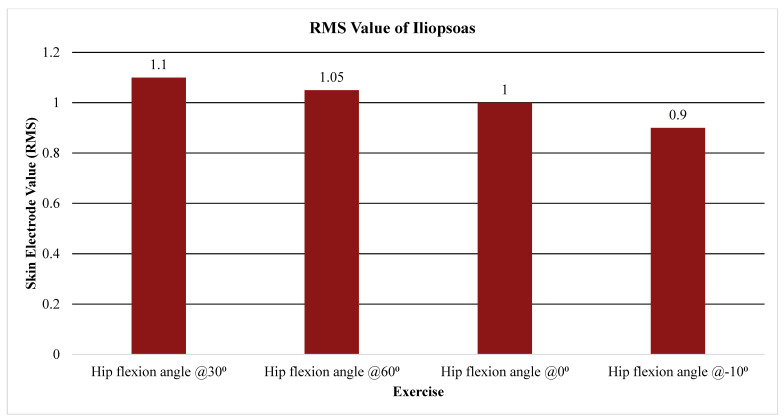
Background/Objectives: The iliopsoas muscle plays an essential role in lumbopelvic and hip anterior stability, which is particularly important in the presence of limited osseous acetabular coverage anteriorly as in hip dysplasia and/or hip micro-instability. The purpose of this systematic review is to (1) describe iliopsoas activation levels during common rehabilitation exercises and (2) provide an evidence-based exercise progression for strengthening the iliopsoas based on electromyography (EMG) studies. Methods: In total, 109 healthy adult participants ranging from ages 20 to 40 were included in nine studies. PubMed, CINAHL, and Embase databases were systematically searched for EMG studies of the psoas, iliacus, or combined iliopsoas during specific exercise. The Modified Downs and Black Checklist was used to perform a risk of bias assessment. PROSPERO guidelines were followed. Results: Nine studies were included. Findings suggest that the iliopsoas is increasingly activated in ranges of hip flexion of 30-60°, particularly with leg lowering/raising exercises. Briefly, >60% MVIC activity of the iliopsoas was reported in the active straight leg raise (ASLR) in ranges around 60° of hip flexion, as well as with supine hip flexion and leg lifts. In total, 40-60% MVIC was found in exercises including the mid-range of the ASLR around 45° of hip flexion and lifting a straight trunk while in a hip flexed position. Conclusions: The findings suggest that exercises in increased hip flexion provide greater activation of the iliopsoas compared to exercises where the trunk is moving on the lower extremity. Iliopsoas activation can be incrementally progressed from closed to open kinetic chain exercises, and eventually to the addition of external loads. The proposed exercise program interprets the results and offers immediate translation into clinical practice.
Keywords: biofeedback; electromyography; exercise therapy; hip flexor; iliopsoas.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Retchford T.H., Crossley K.M., Grimaldi A., Kemp J.L., Cowan S.M. Can Local Muscles Augment Stability in the Hip? A Narrative Literature Review. J. Musculoskelet. Neuronal Interact. 2013;13:1–12. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
