

Malnutrition Diagnosis and Food Consumption in Subacute Post-Stroke Patients During Rehabilitation
- PMID: 39519422
- PMCID: PMC11547535
- DOI: 10.3390/nu16213589
Malnutrition Diagnosis and Food Consumption in Subacute Post-Stroke Patients During Rehabilitation
Abstract
Background: Stroke survivors frequently encounter malnutrition, adversely impacting clinical outcomes. Nevertheless, malnutrition and food consumption in post-stroke patients have not been frequently assessed, and their correlation with rehabilitation outcomes remains inadequately explored. The objective of this observational study was to evaluate malnutrition at admission in these patients, assess food consumption during a six-week rehabilitation program, and analyze their correlation with rehabilitation outcomes.
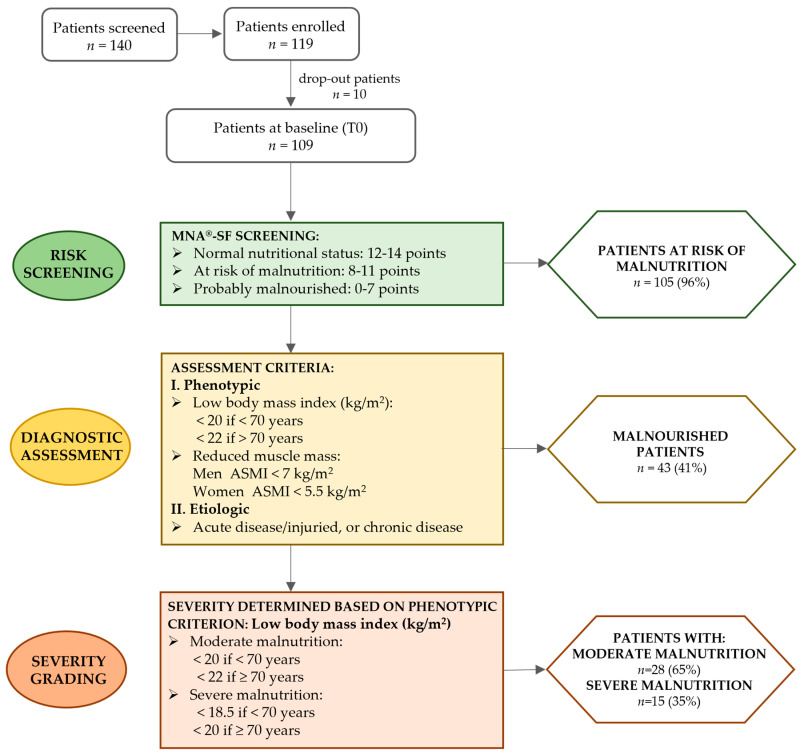
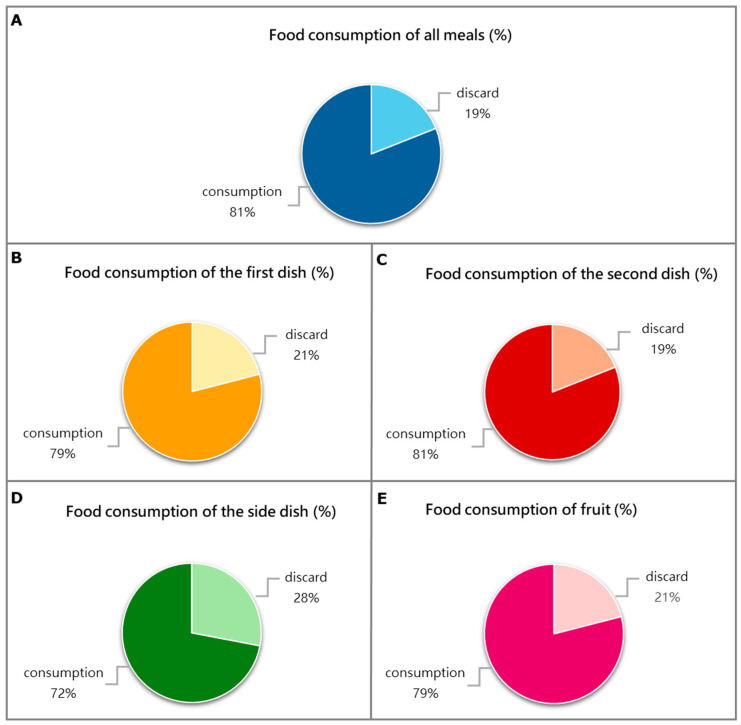
Methods: Subacute post-stroke patients were evaluated at admission (T0) and after a six-week rehabilitation treatment (T1). At T0, we assessed clinical and demographic characteristics, and we diagnosed malnutrition according to the Global Leadership Initiative on Malnutrition (GLIM) criteria. Weight, BMI, hematochemical parameters, and activities of daily living with the modified Barthel Index (mBI) were evaluated at both T0 and T1; recovery was registered as a change in the mBI (ΔmBI = mBIT1 - mBIT0). Patients' food consumption was recorded through visual plate waste estimation of three meals a day, 5 days a week, for six weeks of hospitalization for rehabilitation.
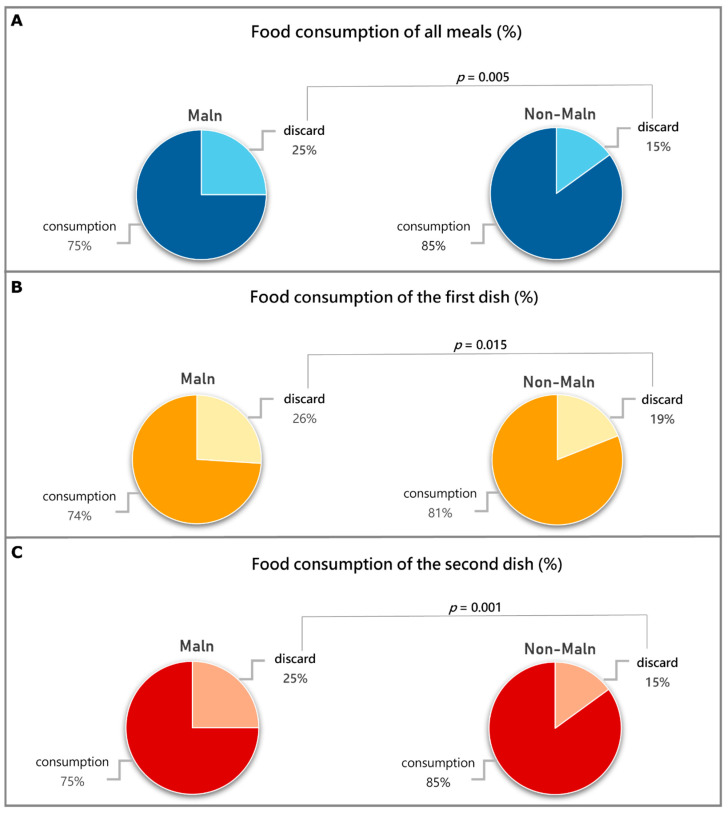
Results: A total of 109 patients completed the study (51 women, mean age 69 ± 11). According to the GLIM criteria, 105 of these patients were at risk of malnutrition, while 43 were malnourished, with 15 severely malnourished. Malnourished patients wasted more food, with respect to non-malnourished patients, as measured by visual plate waste of total meals (25 ± 17% vs. 15 ± 14%; p = 0.001) and reached a lower ΔmBI. A linear regression analysis found a significant correlation between the ΔmBI, the waste of a "second dish", which contained mainly protein, and serum albumin at admission, even after controlling for age.
Conclusions: Malnutrition assessed with the GLIM criteria at admission and food consumption are two important nutritional parameters to evaluate in post-stroke patients hospitalized for rehabilitation due to their association with recovery.
Keywords: GLIM criteria; food consumption; malnutrition; plate waste method; post-stroke; rehabilitation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990-2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1545–1602. doi: 10.1016/S0140-6736(16)31678-6. - DOI - PMC - PubMed
-
- Cederholm T., Jensen G.L., Correia M.I.T.D., Gonzalez M.C., Fukushima R., Higashiguchi T., Baptista G., Barazzoni R., Blaauw R., Coats A., et al. GLIM Criteria for the Diagnosis of Malnutrition—A Consensus Report from the Global Clinical Nutrition Community. J. Cachexia Sarcopenia Muscle. 2019;10:207–217. doi: 10.1002/jcsm.12383. - DOI - PMC - PubMed
-
- Huppertz V., Guida S., Holdoway A., Strilciuc S., Baijens L., Schols J.M.G.A., van Helvoort A., Lansink M., Muresanu D.F. Impaired Nutritional Condition After Stroke from the Hyperacute to the Chronic Phase: A Systematic Review and Meta-Analysis. Front. Neurol. 2021;12:780080. doi: 10.3389/fneur.2021.780080. - DOI - PMC - PubMed
-
- Bernhardt J., Hayward K.S., Kwakkel G., Ward N.S., Wolf S.L., Borschmann K., Krakauer J.W., Boyd L.A., Carmichael S.T., Corbett D., et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Int. J. Stroke. 2017;12:444–450. doi: 10.1177/1747493017711816. - DOI - PubMed
-
- Cereda E., Pedrolli C., Klersy C., Bonardi C., Quarleri L., Cappello S., Turri A., Rondanelli M., Caccialanza R. Nutritional Status in Older Persons According to Healthcare Setting: A Systematic Review and Meta-Analysis of Prevalence Data Using MNA®. Clin. Nutr. 2016;35:1282–1290. doi: 10.1016/j.clnu.2016.03.008. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
