

Genomic insights for personalised care in lung cancer and smoking cessation: motivating at-risk individuals toward evidence-based health practices
- PMID: 39520911
- PMCID: PMC11583727
- DOI: 10.1016/j.ebiom.2024.105441
Genomic insights for personalised care in lung cancer and smoking cessation: motivating at-risk individuals toward evidence-based health practices
Abstract
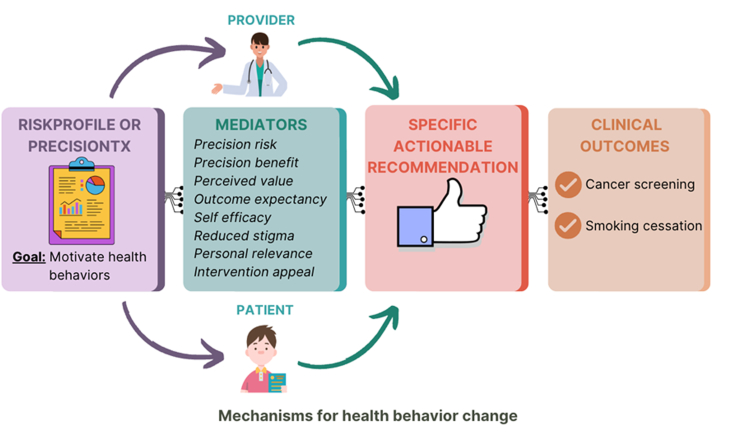
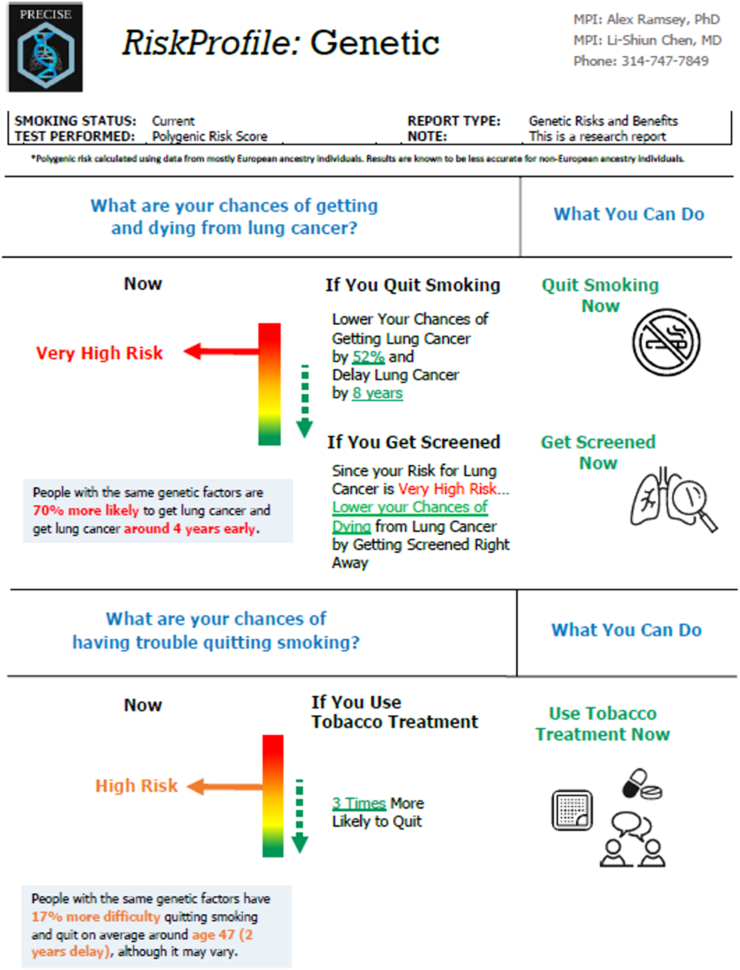
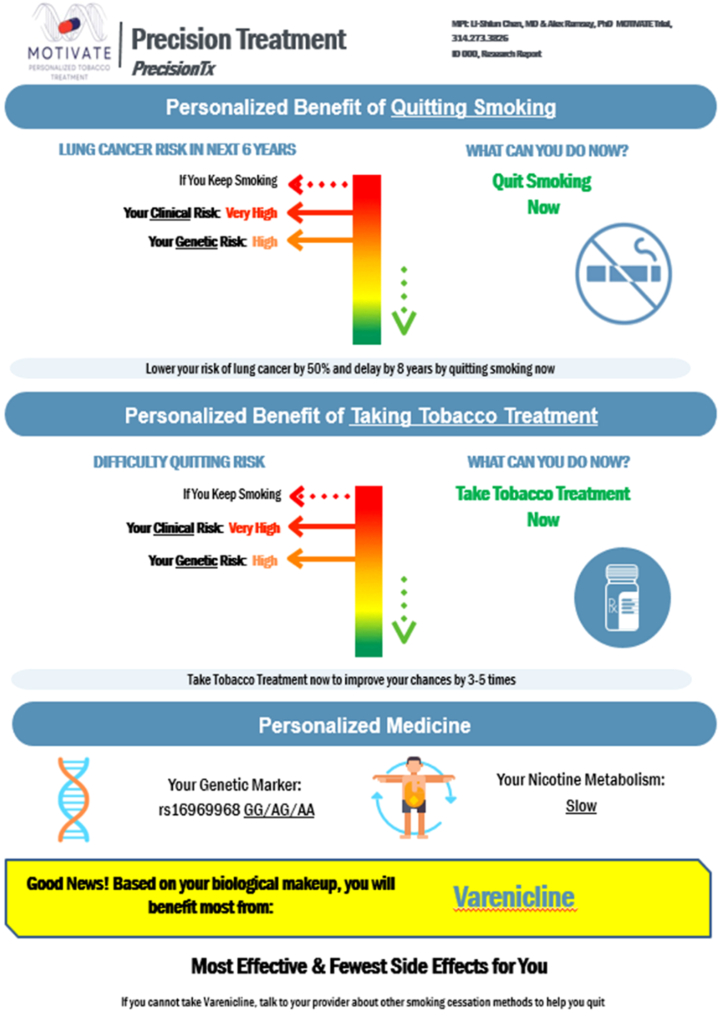
Background: Lung cancer and tobacco use pose significant global health challenges, necessitating a comprehensive translational roadmap for improved prevention strategies such as cancer screening and tobacco treatment, which are currently under-utilised. Polygenic risk scores (PRSs) may further motivate health behaviour change in primary care for lung cancer in diverse populations. In this work, we introduce the GREAT care paradigm, which integrates PRSs within comprehensive patient risk profiles to motivate positive health behaviour changes.
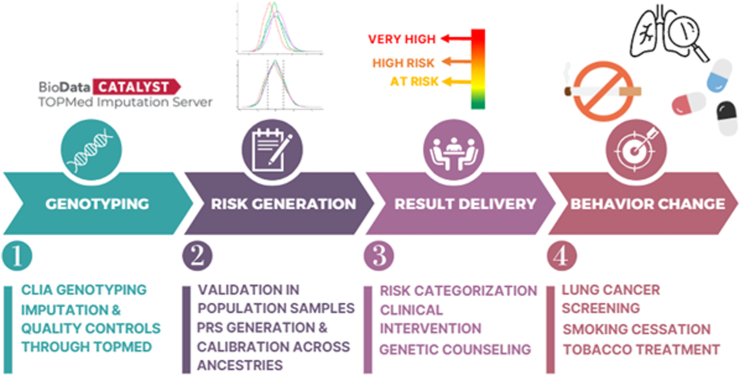
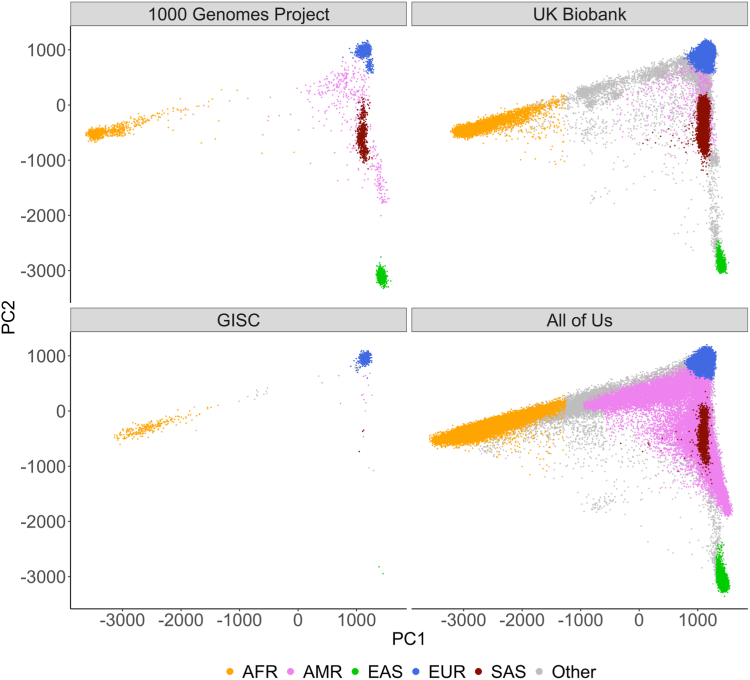
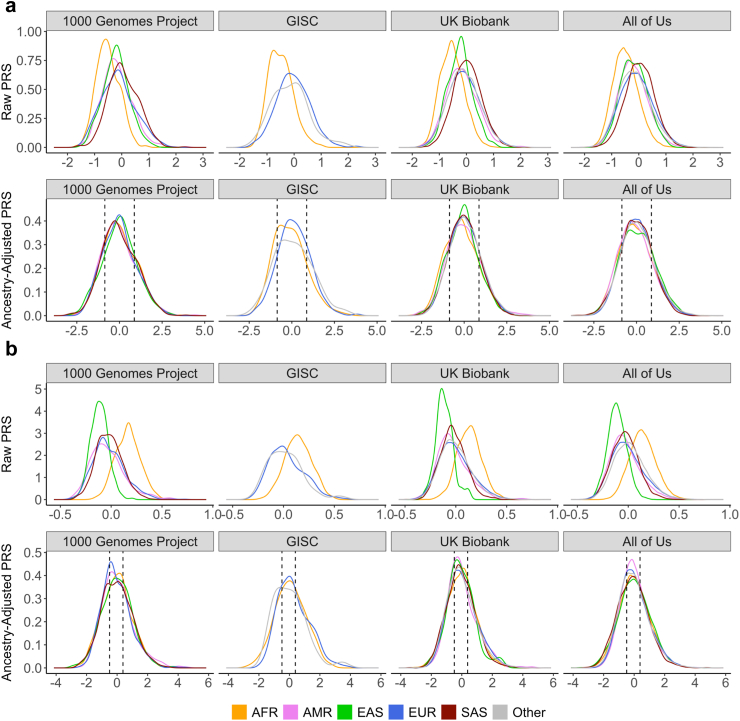
Methods: We developed PRSs using large-scale multi-ancestry genome-wide association studies and standardised PRS distributions across all ancestries. We validated our PRSs in 561,776 individuals of diverse ancestry from the GISC Trial, UK Biobank (UKBB), and All of Us Research Program (AoU).
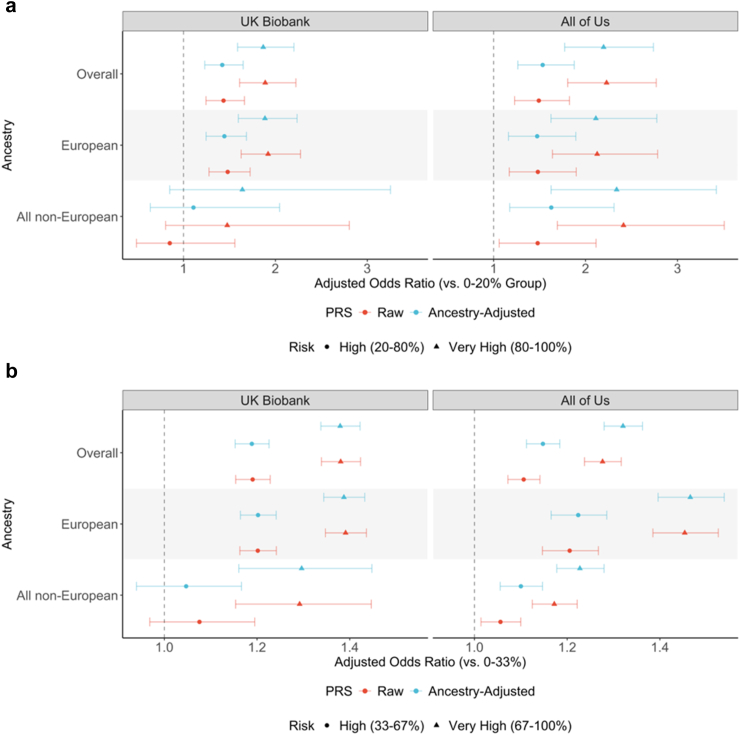
Findings: Significant odds ratios (ORs) for lung cancer and difficulty quitting smoking were observed in both UKBB and AoU. For lung cancer, the ORs for individuals in the highest risk group (top 20% versus bottom 20%) were 1.85 (95% CI: 1.58-2.18) in UKBB and 2.39 (95% CI: 1.93-2.97) in AoU. For difficulty quitting smoking, the ORs (top 33% versus bottom 33%) were 1.36 (95% CI: 1.32-1.41) in UKBB and 1.32 (95% CI: 1.28-1.36) in AoU.
Interpretation: Our PRS-based intervention model leverages large-scale genetic data for robust risk assessment across populations, which will be evaluated in two cluster-randomised clinical trials. This approach integrates genomic insights into primary care, promising improved outcomes in cancer prevention and tobacco treatment.
Funding: National Institutes of Health, NIH Intramural Research Program, National Science Foundation.
Keywords: Cancer prevention; Health behaviour change; Lung cancer; Personalised interventions; Polygenic risk scores; Translational roadmap.
Published by Elsevier B.V.
Conflict of interest statement
Declaration of interests Laura J. Bierut (LJB) is listed as an inventor on Issued U.S. Patent 8,080,371, “Markers for Addiction” covering the use of certain SNPs in determining the diagnosis, prognosis, and treatment of addiction, LJB receives consulting fees from Research Triangle Institute for grant R01DA048824 “Identifying blood-based DNA methylation biomarkers of cannabis use” is a member of US Food and Drug Administration Tobacco Products Scientific Advisory Committee, and co-chair of National Comprehensive Cancer Network Smoking Cessation Panel. Michael J. Bray (MJB) was an employee at ThinkGenetic, Inc, where he had the option to receive stock options at the time the work was conducted. Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy, or views of the International Agency for Research on Cancer/World Health Organization. All other authors have no conflict of interests to report.
Figures
Update of
-
Genomic Insights for Personalized Care: Motivating At-Risk Individuals Toward Evidence-Based Health Practices.medRxiv [Preprint]. 2024 Jun 21:2024.03.19.24304556. doi: 10.1101/2024.03.19.24304556. medRxiv. 2024. Update in: EBioMedicine. 2024 Dec;110:105441. doi: 10.1016/j.ebiom.2024.105441. PMID: 38562690 Free PMC article. Updated. Preprint.
References
-
- Torkamani A., Wineinger N.E., Topol E.J. The personal and clinical utility of polygenic risk scores. Nat Rev Genet. 2018;19:581–590. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
