

Top-Down Proteomics Identifies Plasma Proteoform Signatures of Liver Cirrhosis Progression
- PMID: 39521382
- PMCID: PMC11664408
- DOI: 10.1016/j.mcpro.2024.100876
Top-Down Proteomics Identifies Plasma Proteoform Signatures of Liver Cirrhosis Progression
Abstract
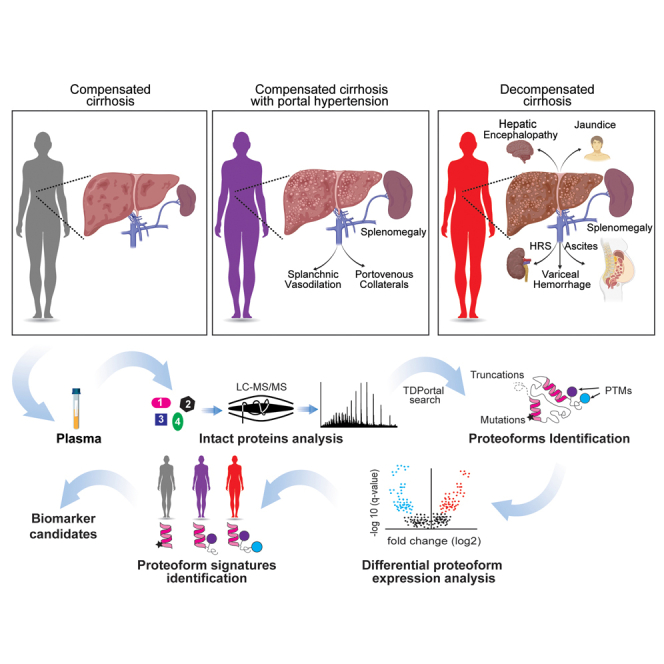
Cirrhosis, advanced liver disease, affects 2 to 5 million Americans. While most patients have compensated cirrhosis and may be fairly asymptomatic, many decompensate and experience life-threatening complications such as gastrointestinal bleeding, confusion (hepatic encephalopathy), and ascites, reducing life expectancy from 12 to less than 2 years. Among patients with compensated cirrhosis, identifying patients at high risk of decompensation is critical to optimize care and reduce morbidity and mortality. Therefore, it is important to preferentially direct them towards specialty care which cannot be provided to all patients with cirrhosis. We used discovery top-down proteomics to identify differentially expressed proteoforms (DEPs) in the plasma of patients with progressive stages of liver cirrhosis with the ultimate goal to identify candidate biomarkers of disease progression. In this pilot study, we identified 209 DEPs across three stages of cirrhosis (compensated, compensated with portal hypertension, and decompensated), of which 115 derived from proteins enriched in the liver at a transcriptional level and discriminated the three stages of cirrhosis. Enrichment analyses demonstrated DEPs are involved in several metabolic and immunological processes known to be impacted by cirrhosis progression. We have preliminarily defined the plasma proteoform signatures of cirrhosis patients, setting the stage for ongoing discovery and validation of biomarkers for early diagnosis, risk stratification, and disease monitoring.
Keywords: LC-MS/MS; apo A-I; fibrinogen alpha chain; haptoglobin; liver cirrhosis; mass spectrometry; proteoforms; top-down proteomics.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest N. L. K. is involved in entrepreneurial activities in Top-down proteomics and consults for Thermo Fisher Scientific. R. D. M. is a current Thermo Fisher Scientific employee. The other authors have declared that they have no conflict of interest with the contents of this article.
Figures





Update of
-
Top-Down Proteomics Identifies Plasma Proteoform Signatures of Liver Cirrhosis Progression.bioRxiv [Preprint]. 2024 Jun 19:2024.06.19.599662. doi: 10.1101/2024.06.19.599662. bioRxiv. 2024. Update in: Mol Cell Proteomics. 2024 Dec;23(12):100876. doi: 10.1016/j.mcpro.2024.100876. PMID: 38948836 Free PMC article. Updated. Preprint.
References
-
- Xu J., Murphy S.L., Kochanek K.D., Bastian B., Arias E. Deaths: final data for 2016. Natl. Vital Stat. Rep. 2018;67:1–76. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
