

Transient biopsy-proven progressive multifocal leukoencephalopathy-immune reconstitution inflammatory syndrome (PML-IRIS) in an elderly woman without known immunodeficiency: a case report
- PMID: 39521972
- PMCID: PMC11549778
- DOI: 10.1186/s12883-024-03945-0
Transient biopsy-proven progressive multifocal leukoencephalopathy-immune reconstitution inflammatory syndrome (PML-IRIS) in an elderly woman without known immunodeficiency: a case report
Abstract
Background: Progressive multifocal leukoencephalopathy (PML) is a severe opportunistic brain disease caused by lytic JC polyomavirus (JCPyV) replication in oligodendrocytes. Although JCPyV infection is common in the general population, PML almost exclusively occurs in patients immunocompromised due to untreated HIV/AIDS, haematological malignancies, primary immunodeficiencies, solid organ transplantation, or immunomodulatory treatment of autoimmune diseases. There is no effective antiviral treatment, and recovery depends on immune reconstitution. Paradoxically, initiation of antiretroviral therapy for HIV/AIDS or interruption of immunomodulating treatment can worsen the clinical manifestations due to immune reconstitution inflammatory syndrome (IRIS). Here, we report an unusual case of spontaneous IRIS in a 76-year-old immunocompetent woman, unmasking PML and leading to unexpected recovery.
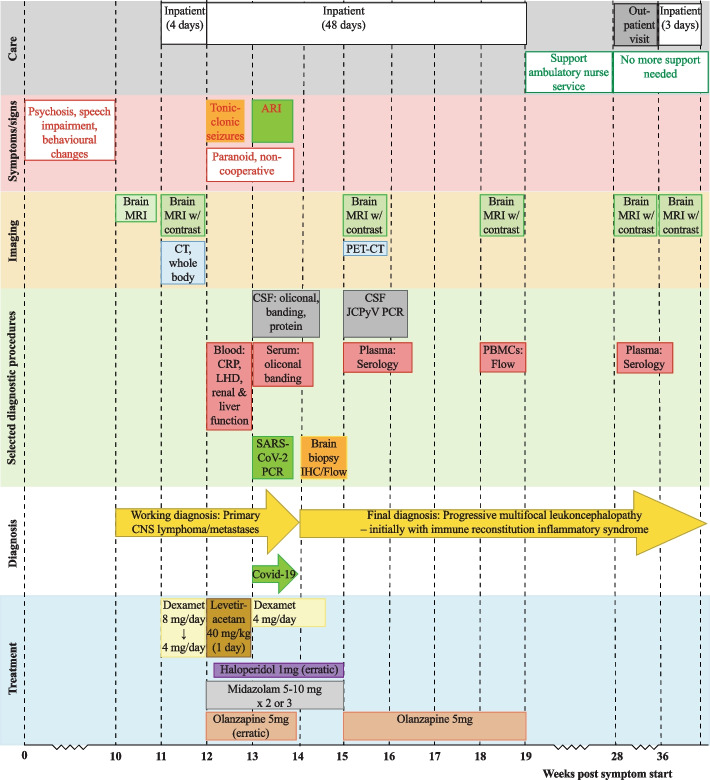
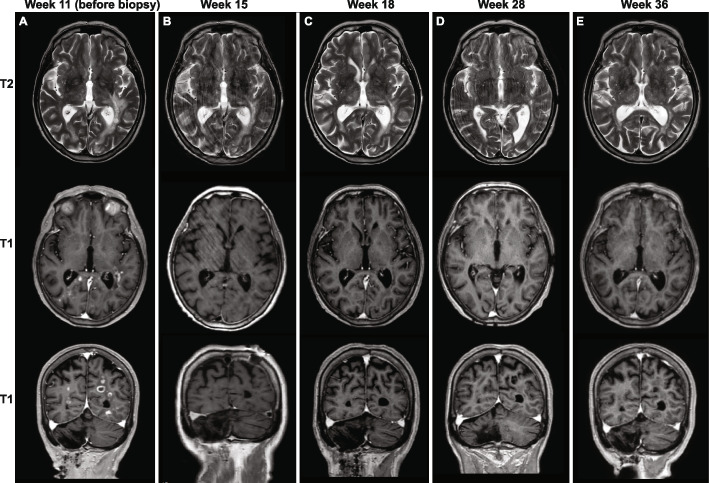
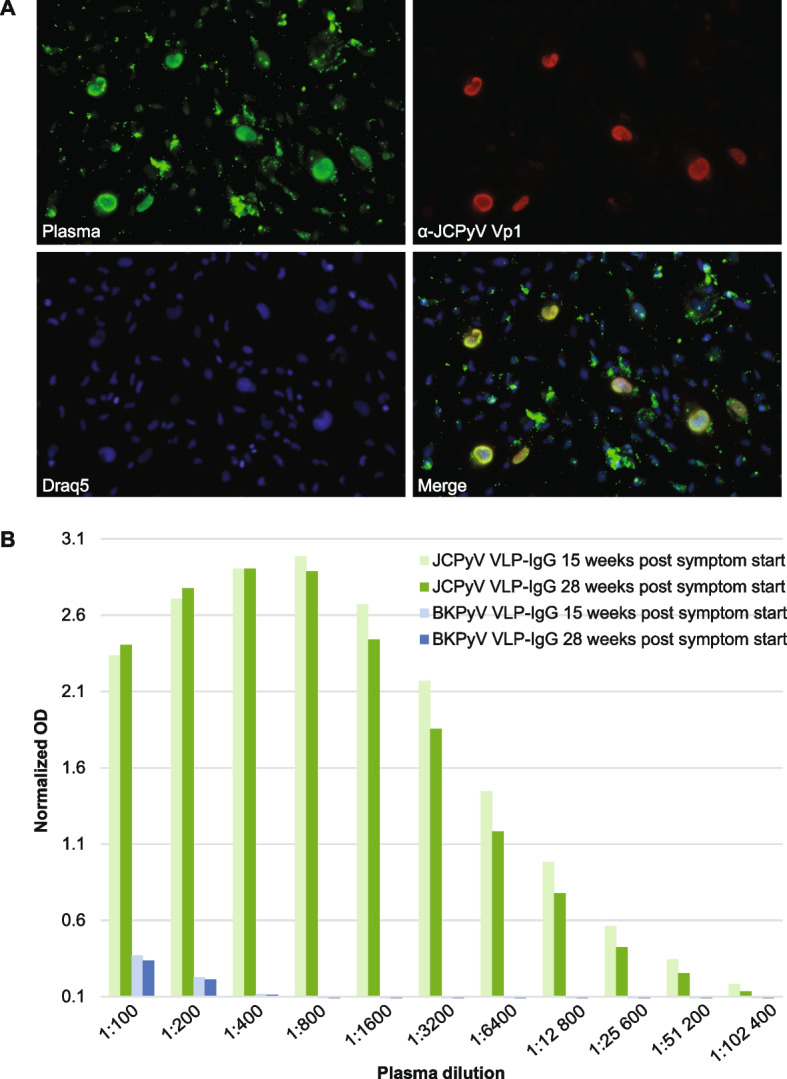
Case presentation: The patient was admitted to the hospital due to psychosis, speech impairment, and behavioral changes over the last three months. She had previously been healthy, except for a cerebellar stroke secondary to paroxysmal atrial fibrillation. Magnetic resonance imaging (MRI) revealed multiple contrast-enhancing white matter lesions suspicious of cancer metastases. Due to suspicion of edema, dexamethasone was administered, and the patient was released while waiting for a stereotactic brain biopsy. Eight days later, she suffered tonic seizures and was readmitted. Intravenous levetiracetam gave rapid effect, but the patient was paranoid and non-cooperative, and dexamethasone was unintentionally discontinued. Ten days later, the brain biopsy revealed demyelination, abundant perivascular T cells, macrophages, and scattered JCPyV-infected oligodendrocytes, rendering the diagnosis of PML-IRIS. The cerebrospinal fluid contained low amounts of JCPyV-DNA, and plasma contained high levels of anti-JCPyV immunoglobulin G. Despite extensive immunological testing, no evidence of immunodeficiency was found. The patient gradually recovered clinically and radiologically. More than 19 months after diagnosis, the patient has only a slight impairment in language and behavior.
Conclusions: An apparently immunocompetent elderly person developed clinically symptomatic PML, which spontaneously resolved with symptoms and signs of IRIS. The atypical MRI lesions with contrast enhancement and the lack of known immunological risk factors for PML delayed the diagnosis, eventually proved by biopsy. PML and PML-IRIS should be considered in the differential diagnosis of patients presenting CNS symptoms and focal lesions with contrast enhancement on MRI.
Keywords: Brain biopsy; CD8 + T cells; Case report; Flow cytometric immunophenotyping; Immune reconstitution inflammatory syndrome; JC polyomavirus; JCPyV antibody; MRI; Macrophages; Progressive multifocal leukoencephalopathy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Hou J, Major EO. Progressive multifocal leukoencephalopathy: JC virus induced demyelination in the immune compromised host. J Neurovirol. 2000;6(Suppl 2):S98–100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
