

Efficacy and safety of inclisiran versus PCSK9 inhibitor versus statin plus ezetimibe therapy in hyperlipidemia: a systematic review and network meta-analysis
- PMID: 39521985
- PMCID: PMC11549808
- DOI: 10.1186/s12872-024-04321-z
Efficacy and safety of inclisiran versus PCSK9 inhibitor versus statin plus ezetimibe therapy in hyperlipidemia: a systematic review and network meta-analysis
Abstract
Objective: Hyperlipidemia plays a crucial role in increasing the risk of cardiovascular diseases such as atherosclerosis. Recent studies have established that inclisiran positively influences lipid regulation. Nevertheless, its effectiveness in comparison to conventional treatments is still questionable. Hence, a methodical assessment of its effectiveness and safety is required. This research evaluates the efficacy and safety of inclisiran, PCSK9 inhibitors, and the combination of statins with ezetimibe in the treatment of hyperlipidemia via a network meta-analysis of randomized controlled trials (RCTs).
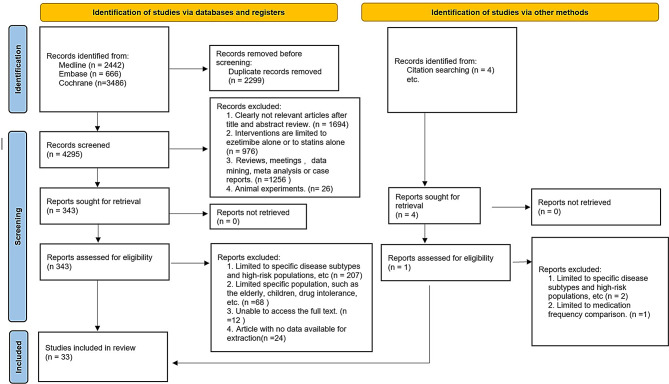
Methods: We performed an extensive search of English-language publications in the PubMed, Medline, Embase, and Cochrane Library databases until April 2024. We conducted a web-based meta-analysis and reported in accordance with the guidelines. We selected the percentage change in low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C) as efficacy evaluation metrics and the incidence of adverse events as safety evaluation metrics for analysis and comparison.
Result: We incorporated 33 studies involving 23,375 patients, evaluating three interventions regarding their effects on LDL-C, TC, TG, HDL-C, and adverse events. All treatments improved metrics over placebo. Inclisiran significantly reduced LDL-C compared to statins (mean - 15.21, 95% CI [-25.19, -5.23]) but showed no significant difference from statin + ezetimibe. Surface under the cumulative ranking curve (SUCRA) rankings placed inclisiran highest for LDL-C reduction (26.2%). The combination of statin and ezetimibe was the most efficacious for triglyceride reduction (mean 17.2, 95% CI [10.22, 24.19]; mean 15.61, 95% CI [16.87, 24.35]). The safety profiles were comparable across treatments.
Conclusion: Inclisiran with its superior LDL-C reduction and low frequency of administration, appears promising for hyperlipidemia treatment, particularly for patients with adherence issues or side effects from other medications.
Systematic review registration: CRD42024550852.
Keywords: A systematic review; Ezetimibe; Hyperlipidemia; Inclisiran; Network meta-analysis; PCSK9 inhibitor; Statin.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






Similar articles
-
Systematic Review and Network Meta-Analysis on the Efficacy of Evolocumab and Other Therapies for the Management of Lipid Levels in Hyperlipidemia.J Am Heart Assoc. 2017 Oct 2;6(10):e005367. doi: 10.1161/JAHA.116.005367. J Am Heart Assoc. 2017. PMID: 28971955 Free PMC article.
-
A Bayesian network meta-analysis of PCSK9 inhibitors, statins and ezetimibe with or without statins for cardiovascular outcomes.Eur J Prev Cardiol. 2018 May;25(8):844-853. doi: 10.1177/2047487318766612. Epub 2018 Mar 23. Eur J Prev Cardiol. 2018. PMID: 29569492 Review.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
PCSK9 monoclonal antibodies for the primary and secondary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2017 Apr 28;4(4):CD011748. doi: 10.1002/14651858.CD011748.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Oct 20;10:CD011748. doi: 10.1002/14651858.CD011748.pub3. PMID: 28453187 Free PMC article. Updated.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.Health Technol Assess. 2008 May;12(21):iii, xi-xiii, 1-212. doi: 10.3310/hta12210. Health Technol Assess. 2008. PMID: 18485273
Cited by
-
Biological and Biosimilar Medicines in Contemporary Pharmacotherapy for Metabolic Syndrome.Pharmaceutics. 2025 Jun 11;17(6):768. doi: 10.3390/pharmaceutics17060768. Pharmaceutics. 2025. PMID: 40574081 Free PMC article. Review.
-
Cardiovascular Risk Assessment and Lipid-Lowering Therapy Recommendations in Primary Prevention.J Clin Med. 2025 Mar 25;14(7):2220. doi: 10.3390/jcm14072220. J Clin Med. 2025. PMID: 40217673 Free PMC article. Review.
-
Therapeutic Inertia in Dyslipidemia Management for Secondary Cardiovascular Prevention: Results from the Italian ITACARE-P Network.J Clin Med. 2025 Jan 14;14(2):493. doi: 10.3390/jcm14020493. J Clin Med. 2025. PMID: 39860503 Free PMC article.
References
-
- Libby P, Buring JE, Badimon L, Hansson GK, Deanfield J, Bittencourt MS, Tokgozoglu L, Lewis EF. Atherosclerosis. Nat Rev Dis Primers. 2019;5(1):56. - PubMed
-
- Karr S. Epidemiology and management of hyperlipidemia. Am J Manag Care. 2017;23(9 Suppl):S139–48. - PubMed
-
- Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, et al. National lipid association recommendations for patient-centered management of dyslipidemia: part 1–full report. J Clin Lipidol. 2015;9(2):129–69. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
