

Validation of a prognostic blood-based sphingolipid panel for men with localized prostate cancer followed on active surveillance
- PMID: 39522029
- PMCID: PMC11550521
- DOI: 10.1186/s40364-024-00678-7
Validation of a prognostic blood-based sphingolipid panel for men with localized prostate cancer followed on active surveillance
Abstract
Background: We previously reported that increases in circulating sphingolipids are associated with elevated risk of biopsy Gleason grade group (GG) upgrading in men on Active Surveillance (AS) for prostate cancer. Here, we aimed to validate these findings and establish a blood-based sphingolipid biomarker panel for identifying men on AS who are at high-risk of biopsy GG upgrading.
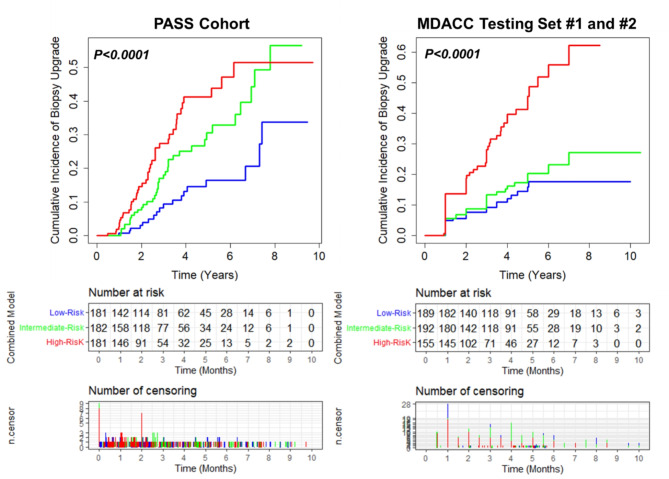
Methods: Men diagnosed with low- or intermediate-risk prostate cancer in one of two AS cohorts (CANARY PASS and MDACC) were followed for GG upgrading after diagnostic and confirmatory biopsy. The PASS cohort consisted of 544 patients whereas the MDACC Cohort consisted of 697 patients. The number of patients with GG upgrading during course of study follow-up in the PASS and MDACC cohorts were 98 (17.7%) and 133 (19.1%), respectively. Plasmas collected prior to confirmatory biopsy were used for mass spectrometry-based quantitation of 87 unique sphingolipid species. A neural network layer based on 21 sphingolipids was developed in the CANARY PASS cohort for predicting biopsy GG upgrading. Tertile-based thresholds for low-, intermediate-, and high-risk strata were subsequently developed for the sphingolipid panel as well as a model that combined the sphingolipid panel with PSA density and rate of core positivity on diagnostic biopsy. The resultant models and risk thresholds for GG upgrading were validated in the MDACC cohort. Performance was assessed using Cox proportional hazard models, C-index, AUC, and cumulative incidence curves.
Results: The sphingolipid panel had a HR (per unit standard deviation increase) of 1.36 (95% CI: 1.07-1.70) and 1.35 (95% CI: 1.11-1.64) for predicting GG biopsy upgrading in the PASS and MDACC cohort, respectively. The model that combined the sphingolipid panel with PSA density and rate of core positivity achieved a HR of 1.63 (95% CI: 1.33-2.00) and 1.44 (1.25-1.66), respectively. Tertile-based thresholds, established in the PASS cohort, were applied to the independent MDACC cohort. Compared to the low-risk group, MDACC patients in the high-risk strata had a GG biopsy upgrade HR of 3.65 (95% CI: 2.21-6.02), capturing 50% of the patients that had biopsy upgrading during study follow-up.
Conclusions: The sphingolipid panel is independently associated with GG biopsy upgrading among men in two independent AS cohorts who have previously undergone diagnostic and confirmatory biopsy. The sphingolipid panel, together with clinical factors, provides a potential means for risk stratification to better guide clinical management of men on AS.
Keywords: Active surveillance; biomarker; prostate cancer; sphingolipids.
© 2024. The Author(s).
Conflict of interest statement
We note that intellectual property was filed related to this work and is pending.
Figures
Similar articles
-
Magnetic Resonance Imaging-Guided Confirmatory Biopsy for Initiating Active Surveillance of Prostate Cancer.JAMA Netw Open. 2019 Sep 4;2(9):e1911019. doi: 10.1001/jamanetworkopen.2019.11019. JAMA Netw Open. 2019. PMID: 31509206 Free PMC article.
-
17-Gene Genomic Prostate Score Test Results in the Canary Prostate Active Surveillance Study (PASS) Cohort.J Clin Oncol. 2020 May 10;38(14):1549-1557. doi: 10.1200/JCO.19.02267. Epub 2020 Mar 4. J Clin Oncol. 2020. PMID: 32130059 Free PMC article.
-
The Impact of Delayed Radical Prostatectomy on Recurrence Outcomes After Initial Active Surveillance: Results from a Large Institutional Cohort.Eur Urol Oncol. 2024 Aug;7(4):838-843. doi: 10.1016/j.euo.2023.11.011. Epub 2023 Dec 5. Eur Urol Oncol. 2024. PMID: 38057193
-
Is magnetic resonance imaging-targeted biopsy a useful addition to systematic confirmatory biopsy in men on active surveillance for low-risk prostate cancer? A systematic review and meta-analysis.BJU Int. 2018 Dec;122(6):946-958. doi: 10.1111/bju.14358. Epub 2018 Jun 6. BJU Int. 2018. PMID: 29679430
-
Outcomes of Grade Group 2 and 3 Prostate Cancer on Initial Versus Confirmatory Biopsy: Implications for Active Surveillance.Eur Urol Focus. 2023 Jul;9(4):662-668. doi: 10.1016/j.euf.2022.12.008. Epub 2022 Dec 23. Eur Urol Focus. 2023. PMID: 36566100 Free PMC article. Review.
Cited by
-
Integrating anamnestic and lifestyle data with sphingolipid levels for risk-based prostate cancer screening.J Transl Med. 2025 Jul 14;23(1):790. doi: 10.1186/s12967-025-06820-9. J Transl Med. 2025. PMID: 40660231 Free PMC article.
References
-
- Sanda MG, Cadeddu JA, Kirkby E, Chen RC, Crispino T, Fontanarosa J, et al. <ArticleTitle Language=“En”>Clinically localized prostate Cancer: AUA/ASTRO/SUO Guideline. Part I: Risk Stratification, Shared decision making, and Care options. J Urol. 2018;199(3):683–90. - PubMed
-
- Klotz L, Vesprini D, Sethukavalan P, Jethava V, Zhang L, Jain S, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol. 2015;33(3):272–7. - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, Metcalfe C, Davis M, Turner EL et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N Engl J Med. 2023. - PubMed
-
- Bruinsma SM, Zhang L, Roobol MJ, Bangma CH, Steyerberg EW, Nieboer D, et al. The Movember Foundation’s GAP3 cohort: a profile of the largest global prostate cancer active surveillance database to date. BJU Int. 2018;121(5):737–44. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
