

Inborn errors of metabolism in neonates and pediatrics on varying dialysis modalities: a systematic review and meta-analysis
- PMID: 39523291
- PMCID: PMC12116838
- DOI: 10.1007/s00467-024-06547-7
Inborn errors of metabolism in neonates and pediatrics on varying dialysis modalities: a systematic review and meta-analysis
Abstract
Background: Some inborn errors of metabolism (IEMs) resulting in aberrations to blood leucine and ammonia levels are commonly treated with kidney replacement therapy (KRT). Children with IEMs require prompt treatment, as delayed treatment results in increased neurological and developmental morbidity.
Objectives: Our systematic review in neonates and pediatrics evaluates survival rates and reductions in ammonia and leucine levels across different KRT modalities (continuous KRT (CKRT), hemodialysis (HD), peritoneal dialysis (PD)).
Data sources: A literature search was conducted through PubMed, Web of Science, and Embase databases for articles including survival rate and toxic metabolite clearance data in pediatric patients with IEM undergoing KRT.
Study eligibility criteria: Cross-sectional, prospective, and retrospective studies with survival rates reported in patients with IEM with an intervention of CKRT, PD, or HD were included. Studies with patients receiving unclear or multiple KRT modalities were excluded.
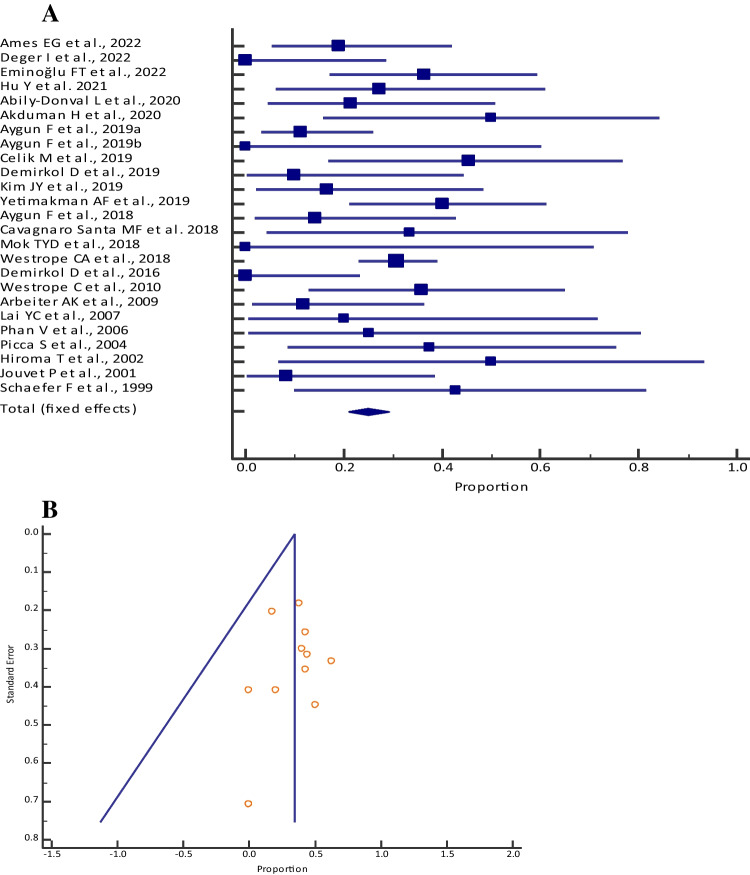
Study appraisal and synthesis methods: Analysis variables included efficacy outcomes [% reduction in ammonia (RIA) from pre- to post-dialysis and time to 50% RIA] and mortality. The Newcastle Ottawa Risk of Bias quality assessment was used to assess bias. All statistical analyses were performed with MedCalc Statistical Software version 19.2.6.
Results: A total of 37 studies (n = 642) were included. The pooled proportion (95% CI) of mortality on CKRT was 24.84% (20.93-29.08), PD was 34.42% (26.24-43.33), and HD 34.14% (24.19-45.23). A lower trend of pooled (95% CI) time to 50% RIA was observed with CKRT [6.5 (5.1-7.8)] vs. PD [14.4 (13.3-15.5)]. A higher mortality was observed with greater plasma ammonia level before CKRT (31.94% for ≥ 1000 µmol/L vs. 15.04% for < 1000 µmol/L).
Conclusions and implications of key findings: Despite the limitations in sample size, trends emerged suggesting that CKRT may be associated with lower mortality rates compared to HD or PD, with potential benefits including prevention of rebound hyperammonemia and improved hemodynamic control. While HD showed a trend towards faster achievement of 50% RIA, all modalities demonstrated comparable efficacy in reducing ammonia and leucine levels.
Prospero registration: CRD42023418842.
Keywords: CKRT; IEM; Neonates; Pediatrics.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Statement of ethics: Not applicable. Consent for publication: Not applicable. Conflict of interest: The authors presented no conflicts of interest.
Figures


Similar articles
-
Home versus in-centre haemodialysis for people with kidney failure.Cochrane Database Syst Rev. 2024 Apr 8;4(4):CD009535. doi: 10.1002/14651858.CD009535.pub3. Cochrane Database Syst Rev. 2024. PMID: 38588450 Free PMC article.
-
Catheter insertion techniques for improving catheter function and clinical outcomes in peritoneal dialysis patients.Cochrane Database Syst Rev. 2023 Feb 22;2(2):CD012478. doi: 10.1002/14651858.CD012478.pub2. Cochrane Database Syst Rev. 2023. PMID: 36810986 Free PMC article.
-
Fenoldopam for preventing and treating acute kidney injury.Cochrane Database Syst Rev. 2024 Nov 28;11(11):CD012905. doi: 10.1002/14651858.CD012905.pub2. Cochrane Database Syst Rev. 2024. PMID: 39607014
-
Non-pharmacological interventions for preventing clotting of extracorporeal circuits during continuous renal replacement therapy.Cochrane Database Syst Rev. 2021 Sep 14;9(9):CD013330. doi: 10.1002/14651858.CD013330.pub2. Cochrane Database Syst Rev. 2021. PMID: 34519356 Free PMC article.
-
Education support services for improving school engagement and academic performance of children and adolescents with a chronic health condition.Cochrane Database Syst Rev. 2023 Feb 8;2(2):CD011538. doi: 10.1002/14651858.CD011538.pub2. Cochrane Database Syst Rev. 2023. PMID: 36752365 Free PMC article.
Cited by
-
Renal replacement therapy in an intensive care unit: guidelines from the SRLF-GFRUP consensus conference.Ann Intensive Care. 2025 Jul 16;15(1):100. doi: 10.1186/s13613-025-01517-0. Ann Intensive Care. 2025. PMID: 40668437 Free PMC article. Review.
References
-
- Jeanmonod R, Asuka E, Jeanmonod D (2024) Inborn errors of metabolism. In: StatPearls. StatPearls Publishing, Treasure Island - PubMed
-
- Amaral AU, Wajner M (2022) Pathophysiology of maple syrup urine disease: focus on the neurotoxic role of the accumulated branched-chain amino acids and branched-chain α-keto acids. Neurochem Int 157:105360. 10.1016/j.neuint.2022.105360 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
