

m5C related-regulator-mediated methylation modification patterns and prognostic significance in breast cancer
- PMID: 39523404
- PMCID: PMC11551150
- DOI: 10.1038/s41598-024-77389-4
m5C related-regulator-mediated methylation modification patterns and prognostic significance in breast cancer
Abstract
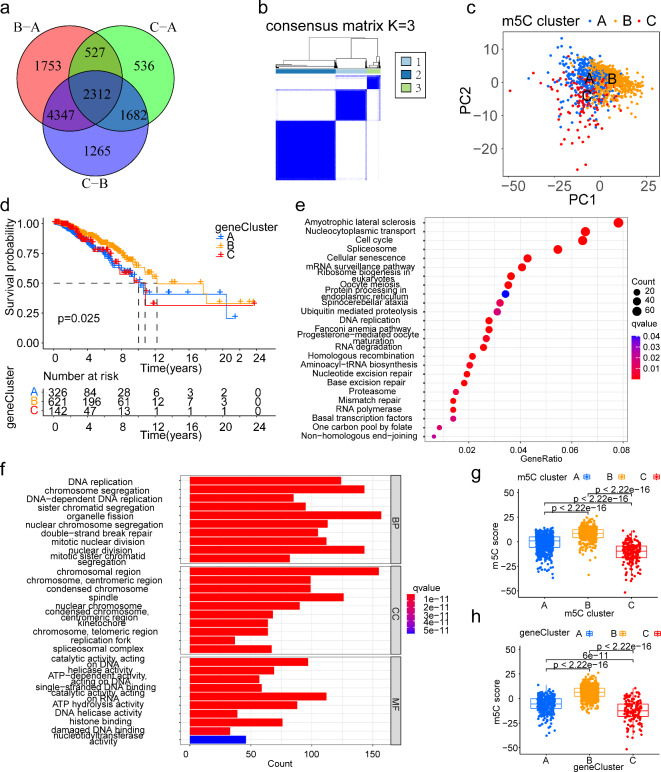
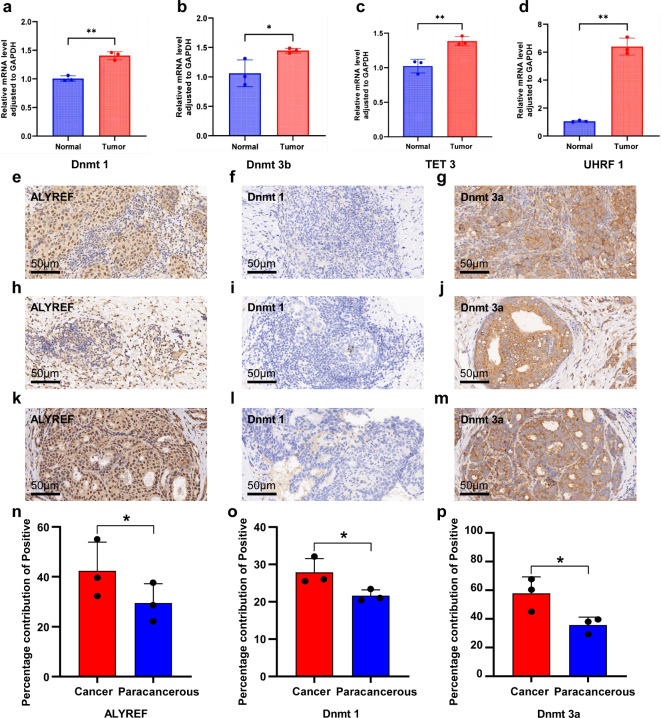
5-Methylcytosine (m5C) is closely associated with cancer. However, the role of m5C in breast cancer(BC)remains unclear. This study combined single-cell RNA sequencing (scRNA-Seq) and transcriptomics datasets to screen m5C regulators associated with BC progression and analyze their clinical values. Firstly, This study elucidates the mechanisms of the m5C landscape and the specific roles of m5C regulators in BC patients. we found that the dysregulation of m5C regulators with m5Cscore play the essential role of the carcinogenesis and progression in epithelial cells and myeloid cells of BC at single cell level. External validation was conducted using an independent scRNA-Seq datasets. Then, three distinct m5C modification patterns were identified by transcriptomics datasets. Based on the m5C differentially expressed regulators, the m5Cscore was constructed, and used to divide patients with BC into high and low m5Cscore groups. Patients with a high m5Cscore had more abundant immune cell infiltration, stronger antitumor immunity, and better prognoses. Finally, Quantitative real-time (PCR) and immunohistochemistry were used for the in vitro experimental validation, which had extensive prognostic value. In this study, we aimed to assess the expression of m5C regulators involved in BC and investigate their correlation with the tumor microenvironment, clinicopathological characteristics, and prognosis of BC. The m5C regulators could be used to effectively assess the cell specific regulation prognosis of patients with BC and develop more effective immunotherapy strategies.
Keywords: Breast cancer; Cell specific regulation; Epigenetics; Immunotherapy; m5C RNA modification.
© 2024. The Author(s).
Conflict of interest statement
Figures





Similar articles
-
Distinct 5-methylcytosine profiles of LncRNA in breast cancer brain metastasis.BMC Cancer. 2025 Mar 27;25(1):557. doi: 10.1186/s12885-025-13948-w. BMC Cancer. 2025. PMID: 40148799 Free PMC article.
-
The hub ten gene-based risk score system using RNA m6A methylation regulator features and tumor immune microenvironment in breast cancer.Breast Cancer. 2022 Jul;29(4):645-658. doi: 10.1007/s12282-022-01341-5. Epub 2022 Feb 16. Breast Cancer. 2022. PMID: 35174450
-
5-Methylcytosine methylation predicts cervical cancer prognosis, shaping immune cell infiltration.J Int Med Res. 2025 Apr;53(4):3000605251328301. doi: 10.1177/03000605251328301. Epub 2025 Apr 12. J Int Med Res. 2025. PMID: 40219803 Free PMC article.
-
Functions and mechanisms of RNA m6A regulators in breast cancer (Review).Int J Oncol. 2024 Sep;65(3):86. doi: 10.3892/ijo.2024.5674. Epub 2024 Jul 26. Int J Oncol. 2024. PMID: 39054967 Free PMC article. Review.
-
Significant roles of RNA 5-methylcytosine methylation in cancer.Cell Signal. 2025 Feb;126:111529. doi: 10.1016/j.cellsig.2024.111529. Epub 2024 Nov 28. Cell Signal. 2025. PMID: 39615772 Review.
References
-
- Sung, H. et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.71, 209–249. 10.3322/caac.21660 (2021). - PubMed
-
- Giaquinto, A. N. et al. Breast Cancer Statistics, 2022. CA Cancer J. Clin.72, 524–541. 10.3322/caac.21754 (2022). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
